
Original Article: JRCRS. 2026:14(2): 71-76
3-Comparison of Mulligan’s Spinal Mobilization with Proprioceptive Neuromuscular Facilitation Technique on Pain, Disability and Range of Motion in Patients with Cervical Radiculopathy: A Randomized Clinical Trial
Azeem Tajdin1
1 Physiotherapist (Neuromuscular), Department of Physical Therapy; Al-Fazal Hospital Nankana Sahib, Punjab, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140203
ABSTRACT:
Background: Cervical radiculopathy involves response, motion and sensational changes e.g. radiating pain, paresthesia, numbness that can be raised by bad positions and motions of neck.
Objective: To determine spinal mobilization and proprioceptive neuro-muscular facilitation comparison on the pain, level of disability and movements ranges in cervical radiculopathy individuals.
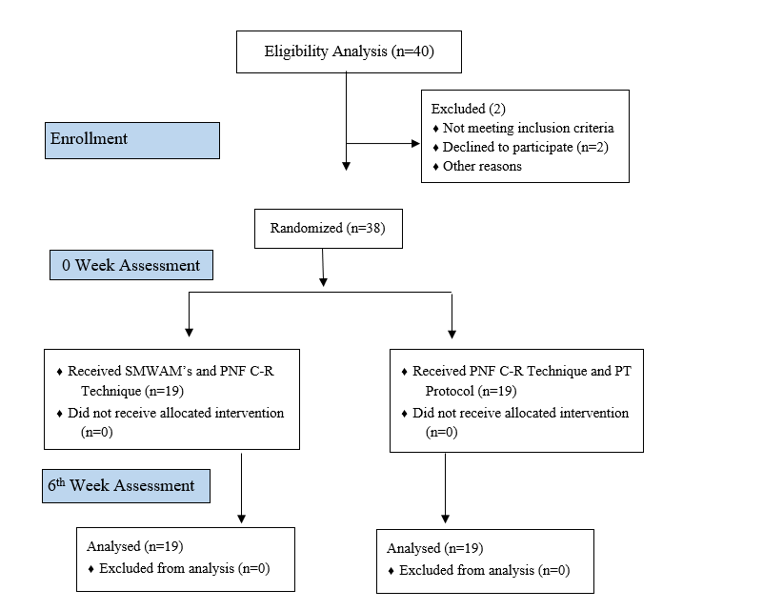
Methodology: The 38 subjects (determined by G*Power 3.1.9.7) divided in 2 groups by lottery method. Control group got Mulligan’s spinal mobilization with arm movements (6 glides three sets) and experimental group received Proprioceptive neuro-muscular facilitation contract relax technique, passive stretching (3 bunches of 10 times repeat) and isometric exercises (2 clusters of 10 times repeat). Numeric pain rating scale for the pain, neck disability index for the level of disability and goniometer for the range of motion outcome measures included. Data analysis was achieved by SPSS (statistical package for social sciences) version 26. (Clinical Trial Registry Number: NCT06866821)
Results: There were 15 males (39.5%), 23 females (60.5%) with right side involved in 24 (63.2%) and left side involved in 14 (36.8%) individuals. The mean, standard deviation of age was 33.95±7.935 years and of duration symptoms were 8.08±1.402 months. There was statistically significant enhancement in NPRS, NDI and cervical ROM pre-& post mean values more in experimental group as compared to control group with P value <0.001.
Conclusion: The individuals managed by proprioceptive neuromuscular facilitation contract relax technique, passive stretching and isometric strengthening exercises had significantly better relief in the pain, level of disability and change in cervical ranges of movements than control group.
Keywords: Cervical Radiculopathy, Pain, Range of motion, Distraction and Proprioceptive neuromuscular facilitation
Introduction:
Cervical radiculopathy involves response, motion and sensational changes e.g. radiating pain, paresthesia, numbness that can be raised by bad positions and motions of neck. Almost 83% of patients regain naturally during 24-36 months, and sequential recovery takes place 4-6 months after start by non-surgical management.1 Cervical radiculopathy (CR) shows pain radiation into upper limb, along with sensation issues like paraesthesia, tingling provoked by neck motion and bad postural habit.2 Pain radiation into upper limb occurs in same side with respect to root of the nerve damaged.3 Neck disc protrusion, osteophyte degeneration lesions might impact sensory fibers resulting paresthesia or numbness, motor fibers of cranial nerve roots resulting lack of active mobility or muscle feebleness and making neuropathic irritation called as burning, shooting, sharp pain or likely electric shock symptoms in the upper limb.4 The most common affected neck nerve roots involve C6, C7; it had been proved due to excessive mobility happening at C5, C6 and C6, C7 levels subjected to maximum biomechanical load and prone to degenerative spondylosis, which narrows the neural foramina.5
Popular causes include spondylosis, intervertebral disc herniation, neck spine instability, osteophytosis, trauma and less commonly cancer causing issues, producing stenosis of space in the vertebral column foramen.6 Cervical radiculopathy novel cases are nearly 107.3 per 1 lac for males yearly and 63.5 per 1 lac for females in 35-50 years old individuals. New cases grow in the 5th life decade to more than 203 per 1 lac. The muscles feebleness occurs in the cervical, scapula, upper arm and hand region.7 Time, laptop type used, woman sex, seeing up at screen unit and task types deficiency are factors that result cervical radiculopathy by aggravated biomechanical stress exposure in routine activities e.g. reading, driving, mobile phones and laptops use with bad posture habits.8 Predisposing factors include Caucasian older age, cigarette smoking, lumbar radiculopathy history and difficult situations are infection, tumour/trauma which can lead to cervical radiculopathy. Physical examination include overlooking at rest, during movement and physical work view e.g. joint work, control of muscle and patterns of movement.9
Electromyography, magnetic resonance imaging are assumed the gold standard for cervical radiculopathy diagnosis but are not available in frequent clinics; due to this Spurling’s test, Distraction test and upper limb nerve tension test for median nerve are performed manually.10 Non-surgical management especially physiotherapy (neck collar, traction), is overall suggested as first management option for cervical radiculopathy.11 Physical therapy is an often used non-surgical treatment in addition to pain medicine for cervical radiculopathy.12 Manual therapy for pain relief includes mobilization, manipulation to the neck and thoracic spine, soft tissue mobilization and neurodynamic methods. Exercise includes making the cervical flexor muscles, thoracic vertebrae and scapular areas powerful. Traction consists of manually by hand, mechanical by assistance and traction in house opportunities.13 Neural sliding or neurodynamic increases the movement by making the stability among the around structures and associated nerve mobility.14 When signs / symptoms radiated from spine to periphery, then mobilization at the respective spinal level should be applied in combination with arm movement.15
Spinal mobilization along with arm movements is a method in which prolonged transverse glide applied to the respective spinal level of the symptomatic vertebrae to no symptoms side meanwhile doing restricted motion actively of surrounding joints. This method is pillared on the awareness i.e. the cervical spine vertebrae, scapula and upper thorax region lead to similar spinal motion.16 Proprioceptive neuromuscular facilitation includes stretching, traction, resisted movement, compression to reduce the atrophy, muscle wasting, and joint movement restriction.17 This method is pillared on the movement patterns to appreciate and correct the sensory, motor work.18 As smart phones, touch pads and laptop screens use is raising in this modern era; cervical pain that radiates in upper arm is also becoming usual because of devices longer time use in risky positions. Objective of study is to find spinal mobilization and proprioceptive neuro-muscular facilitation comparison on the pain; level of disability and movements ranges in cervical radiculopathy individuals. There have been many studies that separately explain the effects of Mulligan’s spinal mobilization and proprioceptive neuro-muscular facilitation on cervical radiculopathy symptoms but limited research has been done on comparison of these treatments. Therefore, the goal of this study is to provide a comparison of both techniques to help physiotherapists choose the more effective option.
Methodology
A randomized clinical trial was conducted at DHQ Hospital and Al-Fazal Hospital Nankana Sahib physiotherapy outpatient department from July 2024 to December 2024. Ethical approval was received from committee of the Riphah College of Rehabilitation & Allied Health Sciences (REC/RCR & AHS/24/0225), Lahore. Sample size is determined by G*Power 3.1.9.7. Effect size (d) 1.30 found with mean, SD of neck disability index 7.1+2.382 in experimental group and 11.55+4.211 in control group based on previous study.19 Due to this, by assuming an alpha error 0.05, power 0.95; a 34 sample size calculated and on adding 10% attrition rate, the total sample size became 38 (19 in each group). Both men and women aged 21–50 years who were diagnosed via imaging by orthopedic specialists and confirmed through three screening tests (upper limb tension, Spurling’s, and distraction tests) were included after providing written informed consent. Conversely, individuals were excluded if they were presented with a history of trauma, fracture, previous surgery, any pathological condition, spinal instability, tumor, vertebrobasilar insufficiency (VBI), or cervical spondylolisthesis.
Subjects divided into 2 groups by lottery method. Control group (N=19) got Mulligan’s spinal mobilization with arm movement (6 glides per set). The horizontal slide should not be left until subject’s arm comes back to starting position. Meanwhile maintaining slide, patient did different movements (flexion/ abduction, horizontal abduction / horizontal adduction) based on previous study.15 All patients got hot pack (10 minutes), active range of motion warm up exercises (2 sets of 10 repetitions) and did isometric neck exercise as a home plan of care. Treatment is provided for 3 days every week in 6 total weeks with 1 meeting per day, 3 bunches of 10 times repeat and resting period of one minute among bunches.
Experimental group (N=19) got the proprioceptive neuro-muscular facilitation contract relax technique with 3 repetitions in each cervical movement (flexion, extension, lateral flexion and rotation),20 passive stretching (3 sets of 10 repetitions) and the isometric strengthening exercises (2 sets of 10 repetitions). Treatment provided 3 days every week in 6 weeks with 1session per day, 5 clusters of 3 times repeat and resting period of one minute among clusters. The outcome measures included numeric pain rating scale for the pain, neck disability index for functional disability and goniometer for movements range at 0 week and after 6th week treatment. The assessor involved in outcome assessment blinded to the group provided. Analysis was performed by SPSS version 26 (statistical package of social sciences). Normality of data evaluated by Shapiro Wilk test. For this normally distributed parametric data; independent t test, one-way Anova test among groups and paired t test within groups utilized.
Results
Out of 38 participants, there were 15 males (39.5%), 23 females (60.5%) with right side involved in 24 (63.2%) and left side involved in 14 (36.8%) individuals. The mean, standard deviation of age was 33.95±7.935 years and of duration symptoms were 8.08±1.402 months, showing moderate cervical radiculopathy in individuals (Table 1). Within groups analysis by using paired sample t test shows significant improvement in the pre & post mean+S.D score of numeric pain rating scale, neck disability index and goniometer cervical range of motions in degrees (P value <0.05 each) among both groups (Table 2). Between group analysis by using independent sample t test shows the statistically significant enhancement in mean+S.D score of numeric pain rating scale (P value <0.031 vs 0.139), neck disability index (P value <0.029 vs 0.144) and goniometer cervical ROM (P value <0.05) more in experimental group as comparatively control group after treatment (Table 3).
| Table 1: Demographic Variables of the Participants | ||||
| Demographic Variables | Control Group | Experimental Group | Total (n=38) | |
| Gender | Male | 6 (31.6%) | 9 (47.4%) | 15 (39.5%) |
| Female | 13 (68.4%) | 10 (52.6%) | 23 (60.5%) | |
| Side Involved | Right | 10 (52.6%) | 14 (73.7%) | 24 (63.2%) |
| Left | 9 (47.4%) | 5 (26.3%) | 14 (36.8%) | |
| Age Mean ± S. D (Years) | 35.63±8.820 | 32.26±6.756 | 33.95±7.935 | |
| Duration Mean ± S. D (Months) | 7.63±1.300 | 8.53±1.389 | 8.08±1.402 | |
| Table 3: Between Group Analysis for NPRS, NDI & Goniometer Cervical ROM | |||||||
| Variable | Movement | Control Group Mean+SD | Experimental Group
Mean+SD |
p-value | Mean Difference | ||
| NPRS | Before Treatment | 5.79+1.47 | 6.47+1.31 | 0.139 | -0.684 | ||
| After Treatment | 2.95+1.35 | 3.79+0.92 | 0.031 | -0.842 | |||
| NDI | Before Treatment | 24.47+4.90 | 27.16+6.11 | 0.144 | -2.68 | ||
| After Treatment | 10.63+4.07 | 14.32+5.75 | 0.029 | -3.68 | |||
| Goniometer Cervical ROM | Flexion Before Treatment | 70.95+7.92 | 66.58+6.19 | 0.07 | 4.37 | ||
| Flexion After Treatment | 80.16+7.07 | 85.05+2.76 | 0.008 | -4.89 | |||
| Extension Before Treatment | 49.58+7.78 | 46.84+7.68 | 0.28 | 2.74 | |||
| Extension After Treatment | 59.37+7.29 | 64.16+5.42 | 0.03 | -4.79 | |||
| Right Lateral Flexion Before Treatment | 31.84+8.78 | 28.74+7.63 | 0.25 | 3.10 | |||
| Right Lateral Flexion After Treatment | 36.42+4.98 | 40.16+2.03 | 0.005 | -3.74 | |||
| Left Lateral Flexion Before Treatment | 35.37+7.42 | 37.05+7.81 | 0.50 | -1.68 | |||
| Left Lateral Flexion After Treatment | 38.58+4.29 | 41.11+2.56 | 0.03 | -2.53 | |||
| Right Rotation Before Treatment | 76.58+8.69 | 71.53+10.66 | 0.12 | 5.05 | |||
| Right Rotation After Treatment | 81.89+4.43 | 84.89+2.40 | 0.01 | -3.00 | |||
| Left Rotation Before Treatment | 76.74+9.06 | 80.95+8.34 | 0.14 | -4.21 | |||
| Left Rotation After Treatment | 81.21+5.31 | 85.68+2.26 | 0.002 | -4.47 | |||
Discussion
The study goal is to determine Mulligan’s spinal mobilization and proprioceptive neuro-muscular facilitation technique comparison on the pain; level of disability and movements ranges in individuals having cervical radiculopathy. The results suggested improvement of groups individually; but there was enhancement of NPRS, NDI or cervical ROM (flexion, extension, right or left lateral flexion, right or left rotation) mean values (p value <0.05) more in the experimental group compared to control group after treatment. The study conducted by Dr. Dhruv Taneja and fellows in 2023 to find efficacy of the spinal mobilization along with limb movements in treatment of one-sided cervical radiculopathy. The findings revealed high improvement in the neck movement ranges (flexion, extension, lateral flexion or cervical rotation) of study group in comparison with control group that revealed a moderate improvement in the neck ranges of motion.15 Current study showed that all variables (NPRS, NDI and Cervical ROM) showed significant improvement in experimental group than control group.
One study was done by Sadaf Shafique and her partners in 2019 to find the effects of Mulligan’s mobilization along with arm movements, neuro-mobilization, and manual traction in cervical radiculopathy individuals. Every group revealed change but study participants revealed much pain relief (NPRS), reduction of disability functional level (NDI) and increase in all movement ranges (goniometry) in the study group rather than other group.21 The current study concluded that NPRS, NDI and Cervical ROM (flexion, extension, right or left lateral flexion, right or left rotation) improved in both groups but all variables much improved in experimental group than control group. One research was conducted by Aida A Nassif and her fellows in 2021 on the efficacy of spinal mobilization along with limb movements on the kinesthetic awareness in patients having severe cervical radiculopathy. The research findings concluded that VAS (sensitive to pain level identification on 10cm line), NDI variables were enhanced in groups but spinal mobilization with arm movements provided much advantage in study group than conventional physiotherapy in other group.19 Current study showed that NPRS (reliable pain readings, easier verbal conversation) and NDI improved significantly in experimental group than control group.
Arbnore Ibrahimaj Gashi and fellows observed effect of the proprioceptive neuromuscular facilitation method on managing cervical radiculopathy in 2023. Comparison of passive stretching and isometric strengthening exercises performed with manual therapy techniques i.e. PNF techniques and passive mobilizations. The VAS2 on day 7 (p value =0.006), VAS3 on day 10 (p value =0.001) showed a huge change in experimental group (passive mobilization along with PNF techniques) by decreasing pain for individuals with cervical radiculopathy.20 According to the current study, NPRS improved in both groups but on comparison, NPRS showed statistically significant change in experimental group than control group. Ahmed S. Kamal and his fellows in 2023 assessed the effect of proprioceptive training paradigm on cervical radiculopathy patients. In control group, neck movements increased and cervical pain decreased. While in experimental group, the change became significant on VAS and CROM device analysis.22 The current study with PNF technique rather than proprioception exercises revealed same that NPRS and Cervical ROM (flexion, extension, right or left lateral flexion, right or left rotation) improved in both groups but showed significant difference of pain and mobility in experimental group than control group. sample size of the study was small, subjects <20 years and >50 years were not added. Data was mostly collected from government hospital OPD and from single city. The study focused on short time duration outcome measures, more than 6 weeks effects were not analyzed. Future research should include large sample size, subjects >50 years old specifically from other cities government, private hospitals and more than 6 weeks prolonged effects.
Conclusion
The results showed that individuals managed by proprioceptive neuromuscular facilitation contract relax technique, passive stretching and isometric strengthening exercises had better significant improvement of pain, level of disability and the cervical movements range in the experimental group as compared to control group which was managed by Mulligan’s spinal mobilization with arm movements.
References
- Thoomes E, Thoomes-de Graaf M, Cleland JA, Gallina A, Falla D. Timing of evidence-based nonsurgical interventions as part of multimodal treatment guidelines for the management of cervical radiculopathy: a Delphi study. Physical Therapy. 2022;102(5):pzab312.
- SHADY N, NEGM HM, ZITOUN ZMY, ABDELHAKIEM NM. Multimodal intervention of high laser with neurodynamic mobilization in cervical radiculopathy. Pjmhs; 2021.
- Rhajib MAN, Islam MW, Hossain MZ, Rahman E. Evidence based physiotherapy management of a cervical radiculopathy patient by using clinical reasoning process. Journal of Spine Research and Surgery. 2022;4(2):54-62.
- Savva C, Giakas G, Efstathiou M, Karagiannis C, Mamais I. Effectiveness of neural mobilization with intermittent cervical traction in the management of cervical radiculopathy: a randomized controlled trial. International Journal of Osteopathic Medicine. 2016;21:19-28.
- Savva C, Korakakis V, Efstathiou M, Karagiannis C. Cervical traction combined with neural mobilization for patients with cervical radiculopathy: A randomized controlled trial. Journal of Bodywork and Movement Therapies. 2021;26:279-89.
- Yun Y-H, Lee B-K, Yi J-H, Seo D-K. Effect of nerve mobilization with intermittent cervical segment traction on pain, range of motion, endurance, and disability of cervical radiculopathy. Physical Therapy Rehabilitation Science. 2020;9(3):149-54.
- Rafiq S, Zafar H, Gillani SA, Waqas MS, Zia A, Liaqat S, et al. Comparison of neural mobilization and conservative treatment on pain, range of motion, and disability in cervical radiculopathy: A randomized controlled trial. PloS one. 2022;17(12):e0278177.
- Ayub A, Osama M, Shakil-ur-Rehman, Ahmad S. Effects of active versus passive upper extremity neural mobilization combined with mechanical traction and joint mobilization in females with cervical radiculopathy: A randomized controlled trial. Journal of back and musculoskeletal rehabilitation. 2019;32(5):725-30.
- Wachidah RN, Herawati I, editors. Physiotherapy management for cervical radiculopathy: A case study. Academic Physiotherapy Conference Proceeding; 2021.
- Rafiq S, Zafar H, Gillani SA, Waqas MS, Zia A, Liaqat S, et al. Effectiveness of neural mobilization on pain, range of motion, and disability in cervical radiculopathy: a randomized controlled trial. 2021.
- Alshami AM, Bamhair DA. Effect of manual therapy with exercise in patients with chronic cervical radiculopathy: a randomized clinical trial. Trials. 2021;22(1):1-12.
- Baumann A, Fisher L, Baumann AN. Addition of McKenzie exercises to a multimodal physical therapy approach for cervical radiculopathy: a case report. Cureus. 2022;14(12).
- Young IA, Pozzi F, Dunning J, Linkonis R, Michener LA. Immediate and short-term effects of thoracic spine manipulation in patients with cervical radiculopathy: a randomized controlled trial. journal of orthopaedic & sports physical therapy. 2019;49(5):299-309.
- Shady N, Negm HM, Zitoun ZY, Abdelhakiem NM. Multimodal intervention of high-intensity laser with neurodynamic mobilization in cervical radiculopathy. Pak J Med Amp Health Sci. 2020;14(4).
- Taneja D, Saharan A, Ranjeeta W, Sharma M, Saharan M, Dubey S, et al. Effect of Mulligan’s Smwam among Subjects with UnilateralCervical Radiculopathy. Eduzone: International Peer Reviewed/Refereed Multidisciplinary Journal. 2023;12(1):11-22.
- Arul Pragassame S, Karthikeyan S, Sarumathi M. Effectiveness of Mulligan spinal mobilization with arm movement (SMWAM) technique along with neurodynamics in cervical radiculopathy patients-An experimental study. 2021.
- Ashfaq M, Babur MN, Malick WH, Hussain MA, Awan WA. Comparative effectiveness of proprioceptive neuromuscular facilitation and passive vertebral mobilization for neck disability in patients with mechanical neck pain: A randomized controlled trial. Journal of Bodywork and Movement Therapies. 2022;31:16-21.
- Bansal R, Paul M. Effectiveness of motor control therapeutic exercise vs. Proprioceptive neuromuscular facilitation in subjects with cervical spondylosis on pain and functional disability. Int J Physiother Res. 2020;8(5):3620-27.
- Nassif AA, Amin FS, Rezkallah SS, Hassan A. Effect of spinal mobilization with arm movements on kinesthetic awareness in patient with chronic cervical radiculopathy: Randomized controlled trial. Fizjoterapia Polska. 2020;20(5):6-11.
- Gashi AI, Kovačič T, Gashi F, Azemi A. The effect of proprioceptive neuromuscular facilitation technique on treating cervical radiculopathy. Journal of Physical Education and Sport. 2023;23(3):722-9.
- Shafique S, Ahmad S, Shakil-Ur-Rehman S. Effect of Mulligan spinal mobilization with arm movement along with neurodynamics and manual traction in cervical radiculopathy patients: A randomized controlled trial. JPMA. 2019;69:1601
- Kamal AS, Zakaria HM, Elsamra MK, Gaballah MA, Elrewainy RM. Efficacy of proprioceptive training paradigm on cervical radiculopathy. Assessment. 2023;1000(2):12.