
Mini Systematic Review: JRCRS. 2026:14(2): 62-70
2-Trends in Physical Therapy Management for Low Back Pain: A Mini Systematic Review of Randomized Controlled Trials
Madiha Anees1, Memoona Bibi2, Huma Balqias3, Iqra Hasib4, Ayesha Khan5, Nimra khan6, Najam ul Haque7, Sunny Anwer8
1 2 Assistant Professor, Rehman Medical Institute, Peshawar, Pakistan
3 Junior Lecturer, Rehman Medical Institute, Peshawar, Pakistan
4-8 Student, Rehman Medical Institute, Peshawar, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140202
ABSTRACT:
Background: Background: Low back pain usually presents below the costal margins and above the inferior gluteal folds i.e., between the 12th rib and the gluteal folds. Globally it has become the leading cause of disability. The lifetime Prevalence of LBP episode varies from 60% to 90%. Many physical therapy treatment options are available for low back pain treatment.
Objective: This mini systemic review study is conducted on trends of physical therapy management in low back pain. In this study the clinical trials and investigative interventions are excluded. Data from different databases was collected to find the management of lower back through exercise.
Methodology: A systematic review was conducted that included 8 databases i-e CINAHL, MEDLINE, PEDro, PubMed, PakMediNet, Cochrane Library, Scopus and Web of Science. Only those RCTs were included in the study that had a minimum score of 6 or above on the PEDro Scale. The articles between the years 2015 to 2025 were included. The search strategy included both key terms and MeSh terms.
Results: A total of 10 studies were included in the systematic review were falling under the inclusion criteria. 4 studies compared different modes of exercise intensities, loads and resistance training. 2 studies compared the effects of manual therapy, one study focused on trunk muscle exercises, one study evaluated the effect of sensorimotor training, and two studies added ankle dorsiflexion and hip strengthening exercises. Out of which 9 studies resulted in 40% to 63% with effect size of 0.4028 reduction in pain and one study resulted in no positive effect on LBP.
Conclusion: The review concludes that physical therapy interventions such as core strengthening with ankle dorsiflexion, hip and trunk exercises, active exercises, manual and massage therapy, and high-load or high-intensity training are effective for managing acute and chronic low back pain, whereas sensorimotor training showed no benefit.
Keywords: Low back pain, Manual therapy, Physical therapy modalities, Musculoskeletal manipulation
Introduction:
Low back pain is muscle tension, stiffness and pain that is localized and present on the posterior aspect of the body from lower margin of the twelfth rib and above the inferior gluteal folds with or without pain referring to one or both limbs lasting at least 24 hours.1,2,3,4 The lumbar spine is present at the lower portion of the vertebral column supporting the biomechanical and gravitational loads while maintaining the alignment in neutral lordotic posture.5 LBP has three apparent sources of pain: 1) radicular pain 2) axial lumbosacral pain 3) referred pain. Radicular leg pain travels along the dermatomal distribution into an extremity secondary to dorsal root ganglion irritation or nerve.4
Chronic LBP is perceived to be a challenging and complex condition with a number of adverse effects like physical disability, psychosocial disruption, disturbed sleep and increased health care costs.6 LBP is the most common musculoskeletal problem seen by physical therapist’s in U.S.A and Australia. Globally it has become the leading cause of disability.7 According to an estimate 5.0% to 10% of acute LBP cases will advance into chronic LBP.8 In the year 2015 the global point prevalence was estimated to be 7.3% of activity limiting LBP, which implies that 540 million people were affected with low back pain.1 The estimated prevalence of LBP in South Asian countries is reported to be (Pakistan 40%, Bangladesh 64%, India 19%, Srilanka 36%).9 With an increasing prevalence rate of 60% to 80% every decade, it is estimated to be as an economic burden in middle and low waged countries.10, 11 Low back pain has also proven to be a major problem in young patients with prevalence of 11.9% +/- 2%. In older adults LBP is acknowledged to be most common, potentially disabling and poorly understood condition with 36% of older patients experiencing an episode of low back ache once a year where 21% reported severe to moderate LBP regularly.6 The life time incidence of an acute LBP epsiode vary from 60% to 90% while 30% of those with LBP may develop a chronic condition that may cause significant functional limitations.12
Symptoms of LBP can derive from a number of potential sources such as fascia, bones, inter vertebral discs (IVD’s), muscles, joints and organs of abdominal cavity.13 Low back pain symptoms peaks in ages between 40 and 69 years and is more common among females than males in all age groups.7
Many physical therapy treatment options are available for low back pain including heat and cold therapy, ultrasound, traction, exercise therapy, manual mobilization and manipulation, electro therapy and patient education.14
Evidence showed that the thrust or manipulation interventions can reduce the pain intensity with some active comparators for example exercise. Also, mobilization or non thrust interventions have minimal effects in decreasing the pain.15 A study was performed to see the effectiveness of ultrasound therapy on the management of chronic nonspecific low back pain, concluded that ultrasound therapy helps in decreasing the intensity of pain.16 Traction is the use of force to distract joints and tissues helps in decreasing the intensity of pain.17 A systematic review concluded that routine exercise therapy when compared with core stabilization exercise therapy is less effective in decreasing the pain in patients with non specific low back pain.18
According to a systematic review majority of the high quality researches prefer the non-invasive conservative management for the treatment of low back pain and recommend physical exercises, manual therapy, staying active, patient education and the use of NSAIDS and paracetamol.19,20 A systematic review concluded beneficial effect for coordination/stabilization and strength exercise program over other non-conservative treatments of chronic LBP.21 A study showed that pain, quality of life, disability and avoidance of fear can be improved by active walking or exercise in chronic low back pain.22
This systemic review study is conducted on trends of physical therapy management in low back pain. In this study the clinical trials and investigative interventions are excluded. Data from different databases will be collected to find the management of lower back through exercise.
Methodology:
This study includes searching through multiple databases (i.e. CINAHL, PUBMED, PEDro, MEDLINE, Pakmedinet, Cochrane Library, Scopus and Web of Science) dated from 5th april,2025 to 12th july,2025. The author’s conducting the review thoroughly by searching through all the databases to find the most relevant articles. The searching strategy used by authors to find suitable articles included the use of both key and Mesh words. Following table shows the search terms used for CINAHL.
The authors also made use of the Boolean logical operators (AND & OR) in their search in the above-mentioned databases to broaden or narrow up the articles. The Boolean logical operators were used in the following method. Low back pain AND Manual therapy AND Combined modality therapy. Low back pain OR Manual therapy OR Combined modality therapy. Low back pain AND Manual therapy AND Combined modality therapy. Low back pain AND Manual therapy AND Combined modality therapy.
The PEO framework was used by the authors to assist in the inclusion and exclusion criteria of the study where P: Population, E: Exposure and O: Outcomes. The population included in the study was individuals suffering from Acute or Chronic and Specific or Nonspecific low back pain (The pain experienced was localized and present below the costal margins and above the inferior gluteal folds).
The exclusion criteria enlisted individuals who had undergone through any type of lumbar or hip surgery, spinal fusion, lumbar radiculopathy, spinal cord injury, disability, tumor, systemic inflammatory disease or osteoarthritis. Pregnant or women with postpartum low back pain were also excluded.
The authors only included randomized control trials (RCT) in their systematic review to analyse the effects of different exercise techniques and modalities on low back pain. The articles were selected from the year 2015 to 2025, were in English language, available in full text, used Visual Analogue Scale (VAS) or Numeric Pain Rating Scale (NPRS) were included in the study.
Quality assessment of the research articles is an essential element while conducting a systematic review. Many scales are available that can be used to assess the quality of a randomized control trial. The tool that we used to critically appraise the extracted articles was PEDro Scale. It was developed by PEDro user to identify trails that have sufficient statistical information and are internally valid. The PEDro scale enlists eleven (11) points with a total score of 10.
On the basis of these points, an RCT article can be categorized into the 4 types i.e., Poor (0-3), Fair (4-5), Good (6-8) and Excellent (9-10).
Results
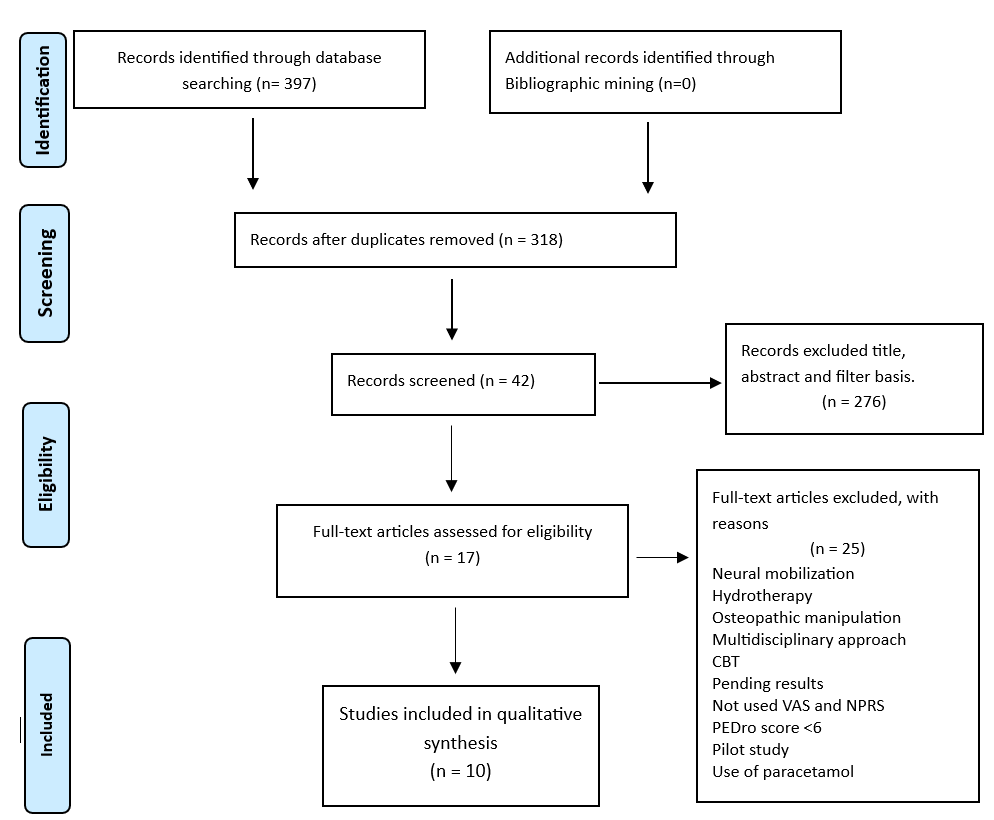
The search strategy performed by the author’s was applied to each database and relevant research studies were identified. The number of articles gathered was at a total of 397 out of which 318 were left and 79 articles were removed after the process of duplication. In the next step, a total of 42 were left after a thorough screening of all the titles, abstracts and applying relevant search filters.
After assessing the full text articles with a total number of 42, 10 articles were selected that were fulfilling the inclusion and exclusion criteria. Remaining 25 articles were excluded as they were coming under the exclusion criteria. The 10 articles that were selected were also critically appraised by the authors using the PEDro scale out of which 10 articles, which were coming under the category of ‘Good’ and ‘Excellent’.
The studies gathered in the review were conducted in 7 different countries i.e. Pakistan (n=1), France (n=1), Belgium(n=2), Sweden(n=1), Italy(n=1), South Korea(n=1), Florida(n=1), Australia (n=2) and Switzerland (n=2). The studies reviewed only included randomized control trials and the common objective among the studies was the management of low back pain. The studies include in the review were conducted from the year 2011 to 2020, where mean age of the patient’s including both male and females was ranging 18 and 85 years with the sample size varying from a total of 25 to 80.Table 2 Data Extraction with articles
To assess the risk of biasness in the methodological quality of the studies included the authors used PEDro scale. Only those studies were included in the review that were falling under the category of ‘good’ and ‘excellent’ I-e having a score of ‘6-10’.
A total number of 10 studies were included in the review, which had the common aim of managing the effects of different physiotherapy techniques on the intensity of pain and disability caused by the chronicity of low back pain. The studies included by the authors had a score of 6 or above on the PEDro scoring scale. The results obtained by all these studies were calculated using either visual analogue scale (VAS) or numeric pain rating scale (NPRS). Or both the scales were used to check the effect of different techniques on pain intensity. VAS which had the scoring criteria of 0-10 or 0-100mm were included.
Out of the 10 studies, 4 focused on the exercise intensity, resistance and load lifting. The study that used total body resistance training calculated a significant 63% decrease in the pain with a mean score of 4.1-5.9(NPRS) in 4 months. Another study stated that there was 56% improvement in decreasing pain with a 3.2 point reduction on NPRS in the high intensity training group as compared to the moderate intensity group. Two studies compared high load or high intensity and low load or low intensity showed no significant changes between the group analysis but the reduction in pain intensity was overall calculated from 39% to 80%.
The results of a study illustrate that clinical and therapeutic effects of core stabilization exercise program over the period of six weeks are more effective in terms of reduction in pain, compared to routine physical therapy exercise for similar duration. This study found significant reduction in pain across the two groups at 2nd, 4th and 6th week of treatment with p value less than 0.05. There was a mean reduction of 3.08 and 1.71 on VAS across the core stabilization group and routine physical therapy exercise group respectively.
One study that compared the effect of addition of hip strengthening with lumbopelvic exercise and lumbo-pelvic exercise alone reported 68% change with 25-point decrease on VAS in the group which had lumbopelvic with hip strengthening exercise.
The other study compared drawing to the abdominal wall with addition of ankle dorsiflexion and drawing to the abdominal wall as novel core stabilization technique for treating LBP. The addition of dorsiflexion was proved to be 50% more effective with a drop of 6.30 to 3.35 on VAS.
Authors also included two studies which focused on the effects of manual or massage therapy on treating low back pain. One study concluded that the new rehabilitative massage programme was more effective with a score of 1.87-1.24 on VAS than the traditional massage therapy. The other study concluded that manual therapy was more effective with a mean of 23-17 on VAS as compared to sham treatment.
A study was included by the authors who compared the effects of sensorimotor training with sham exercises resulted in 6.6mm decrease on VAS in the sham exercise group.
A study which compared the effects of specific trunk exercises with general exercises on low back pain was also included by authors. It resulted in significant decrease in pain in the specific trunk exercises group.
| Table 2: Data Extraction with articles | |||||
| Title | Year of study | Outcome measures | Patient information | Methodological quality | Results |
| Effectiveness of core stabilization exercises and routine exercise therapy in management of pain in chronic non-specific low back pain: A randomized controlled clinical trial | 2015 | Visual Analogue Scale | Both men and women
20-60 years Population= 120 |
8/10 | Specific Trunk Exercise Group (SEG) resulted in Significant Reductions in Pain and Disability as compared to General Exercise Group. |
| Regional manual therapy and motor control exercise for chronic low back pain: a randomized clinical trial
|
2018 | Disability level, pain intensity, pain catastrophizing, fear avoidance beliefs, and perceived effect of treatment | Both men and women
20-65 years Population= 46 |
6/10 | standard physical therapy with or without regional manual therapy resulted in significant improvements in disability level, pain intensity, pain catastrophizing, and fear avoidance beliefs over 12 weeks in persons with chronic low back pain and movement coordination impairments. |
| Core Stability and Hip Exercises Improve Physical Function and
Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial |
2020 | The passive straight leg raising test
Numeric Pain Rating Scale Visual Analogue Scale toe-touch test Straight Leg Raise |
Both male and female
>18 years Population= 75 |
6/10 | Core stability exercise and hip muscle stretching are effective at improving physical function and activity in non-specific LBP patients |
| The effect of the addition of hip strengthening exercises to a lumbopelvic exercise programme for the treatment of non-specific low back pain: A randomized controlled trial. | 2015 | Visual Analogue Scale
Oswestry Disability Index |
Both male and female
18-65 years Population= 80 |
8/10 | Both exercises programmes had concluded similar efficacy results in decreasing pain and disability. |
| Neuromuscular Control and Resistance Training for People with Chronic Low Back Pain: A Randomized Controlled Trial | 2024 | Numeric Pain Rating Scale
Oswestry Tampa Scale for Kinesiophobia, Pain Self-Efficacy Questionnaire, and the International Physical Activity Questionnaire. |
Both male and female
18-65 years Population= 69 |
6/10 | Adding lumbar neuromuscular control retraining to a series of resistance exercises offered no additional benefit over resistance exercises alone over a 12-week period |
| High load lifting lifting exercise and low load motor control exercises as interventions for patients with mechanical low back pain: A randomized controlled trial. | 2016 | Visual Analogue Scale
Rolland Morris Disability Questionnaire |
Both male and female
25-60 years Population= 70 |
8/10 | Between 50% to 80% participants reported decrease in pain intensity. Whereas no difference was observed between the two groups. |
| The efficacy of a preparatory phase of a touch-based approach in treating chronic low back pain: A randomized controlled trial. | 2017 | Visual Analogue Scale
McGill Pain Questionnaire Waddle Disability Index |
Both male and female
30-60 years Population= 51 |
6/10 | The new massage approach as compared to the traditional approach was proved to be more effective in reducing pain. |
| Postural sensorimotor training versus sham exercise in physiotherapy of patients with chronic non-specific low back pain: An exploratory randomized controlled trial. | 2018 | Visual Analogue Scale
Oswestry Disability Index |
Both male and female
>18 years Population: 25 |
8/10 | Sensorimotor training added slight to no benefit in reducing pain and disability in patients with moderate low back pain. |
| Exercise intensity matters in chronic nonspecific low back pain rehabilitation.
|
2019 | Numeric Pain Rating Scale
Modified Oswestry Disability Index Patient Specific Functioning Scale Cardiopulmonary exercise test |
Both male and female
25-60 years Population= 38 |
7/10 | High intensity training was proved to be more effective, feasible and tolerated than moderate intensity training in people with CNSLBP. |
| High intensity training to treat chronic non-specific low back pain: Effectiveness of various exercise modes.
|
2020 | Numeric Pain Rating Scale
Patient Specific Functioning Scale Modified Oswestry Disability Index |
Both men and women
25-60 years Population: 80 |
7/10 | Improvements were resulted after the high intensity training was added in all the groups. Whereas the between group comparison has similar results in reducing pain. |
Discussion
The purpose of this systematic review conducted by the authors was to find out the latest physical therapy trends in managing acute or chronic and specific or nonspecific low back pain due to its high prevalence rate. Articles from different databases were searched and relevant articles were included in the study which had the same goal of decreasing pain through different techniques. The results of which concluded that applying different techniques in managing low back pain were mostly effective.
A total of 10 studies met our inclusion criteria which were included in the systematic review by the authors. The study population included both males and females who had either acute or chronic low back pain and were conducted in different countries all around the world mostly in Europe.
A study compared the effects of novel core stabilization technique with the addition of dorsiflexion. It was in 8-week intervention study which included drawing in the lower abdomen below the navel with a pressure biofeedback unit attached on the lumbar spine when patient was lying in supine position. A target pressure of 40mmHg was required. The experimental group received this treatment along with the addition of dorsiflexion. The result concluded that the addition of dorsiflexion had better results in decreasing pain, physical disability and increasing core stability in patients with chronic low back pain.23 In comparison to which a study suggested that with 60 participants also performed the abdominal drawing in manoeuvre along with resisted dorsiflexion (5 session per week) suggested same beneficial effects of addition of ankle dorsiflexion in abdominal drawing in manoeuvre in the management of chronic low back pain.24
Hip strengthening exercises as an addition to lumbopelvic exercises that included an education session, rehabilitation session including ultrasound training and home-based exercise program resulted in Favor of the addition of hip strengthening exercise to the normal exercise program. It was proved to be more effective in the treatment of non specific low back pain.25 In Favor of which a study conducted in 2020 also concluded that the addition of core stability and hip exercises that includes hip muscle stretching and strengthening with isometric contraction had greater effects on low back pain.26
Moreover, a study included in this systematic review suggested that sensorimotor training adds no benefit in the treatment of low back pain.27 However, sensorimotor training along with ultrasound therapy, Kinesio taping and peripheral neuromuscular facilitation techniques showed improvement in treating low back pain.28
Additionally, specific trunk exercises that is, whole body stretching, side and prone lying trunk exercises hip specific exercises , skilled abdominal and postural training was effective in decreasing pain and improving postural impairment in people with chronic low back pain.29 In Favor of which a study that included 10 sessions of trunk exercises combined with flexibility exercises for 5 weeks (twice a day, 60 minutes per session) also concluded similar beneficial results in the treatment of LBP.30
As mentioned earlier, manual therapy was proved to be clinically relevant when performed with active exercises in the treatment of low back pain. Manual therapy group received 8 therapeutic sessions that included passive accessory intervertebral movements, muscle energy techniques, hold relax techniques, high velocity low amplitude thrust for 30 minutes per session.31 As well as the new rehabilitative massage program that includes surface and deep touch, static and dynamic pressure and pinching and rolling also resulted in better effects in decreasing pain perception in the people suffering from chronic low back pain.32
In accordance with this theory, 2 studies compared the effects of high intensity training with moderate intensity on the patients suffering from LBP. A 12 week program that consisted of 24 therapy sessions concluded that cardiorespiratory training, general resistance (vertical traction, leg curl, chest press, leg press, arm curl, leg extension) and core muscle training (glute bridge, lying diagonal back extension, knee plank, knee side plank, elastic band shoulder retraction with hip hinge) all performed at high intensity shows greater levels of improvement in decreasing pain.33 In support of which another study conducted in 2020 states the same beneficial effects of high intensity training of different exercises on the patients suffering from lower back pain.34
A high load lifting exercise group consisting of 35 participant performed deadlifts following the Valsalva manoeuvre. The load was gradually increased, that helped in activating the stabilizing muscles while the lumbar spine was held in neutral position by the subject. This study consisted of 12 treatment sessions over an 8-week period. The results were in Favor of high load lifting exercise as it decreases the levels of pain perception and disability in patients suffering from mechanical low back pain.35 A study in 2014 concluded that total body resistance exercises that include leg press, leg curl, chest press, chest extension, seated row, overhead press, triceps dip, lumbar extension, bicep curl, calf press, abdominal curl and lumbar extension exercise were more beneficial in reducing pain than lumbar extension exercise alone in patients suffering from low back pain.36
Strengths and limitations: With regards to the strengths of this mini review the quality of all the studies included were assessed using the PEDro scoring scale in which only those studies were included which had the minimum score of 6 or above. Lastly the systematic review was conducted using the PRISMA guidelines.
On the other hand, because of the limitation of time we could only include the articles from the year 2011 to 2021.The studies that were only published in English language and the studies that only targeted lumbar pain. The scales included were VAS and NPRS. The study in not registered on PROSPERO and the review is a mini systematic review.
Recommendations: To further strengthen the study, other researchers can also include articles published before 2011, articles published in other languages and the articles that included the association of lower back with any other region. Studies that used other pain measuring scale can also be included.
Conclusion
Based on the above results the systematic review conducted by the authors concludes that physical therapy techniques including novel core strengthening exercises with the addition of ankle dorsiflexion, hip strengthening exercises, specific trunk exercises along with active exercises, manual and massage therapy techniques, high load lifting exercises or high intensity training exercises were proved to be effective in the treatment of acute or chronic low back pain. On the contrary, sensorimotor training resulted to be non beneficial in the management of low back pain.
References
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. The Lancet. 2018;391(10137):2356-67.
- McIntosh G, Hall H. Low back pain (acute). BMJ clinical evidence. 2011;:1102.
- Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Annals of the rheumatic diseases. 2014;73(6):968-74.
- McIntosh G, Hall H. Low back pain (acute). BMJ clinical evidence. 2011;.
- Cheng JS, Carr CB, Wong C, Sharma A, Mahfouz MR, Komistek RD. Altered spinal motion in low back pain associated with lumbar strain and spondylosis. Evidence-based spine-care journal. 2013;4(01):006-12.
- Jones LD, Pandit H, Lavy C. Back pain in the elderly: a review. Maturitas. 2014;78(4):258-62.
- Learman KE, Ellis AR, Goode AP, Showalter C, Cook CE. Physical therapists’ clinical knowledge of multidisciplinary low back pain treatment guidelines. Physical Therapy. 2014;94(7):934-46.
- Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Revista de saude publica. 2015;49:73.
- Khan MNU, Morrison NM, Marshall PW. The Role of Fear-Avoidance Beliefs on Low Back Pain-Related Disability in a Developing Socioeconomic and Conservative Culture: A Cross-Sectional Study of a Pakistani Population. Journal of Pain Research. 2020;13:2377.
- Calvo-Muñoz I, Gómez-Conesa A, Sánchez-Meca J. Prevalence of low back pain in children and adolescents: a meta-analysis. BMC pediatrics. 2013;13(1):1-12.
- Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A systematic review of the global prevalence of low back pain. Arthritis & Rheumatism. 2012;64(6):2028-37.
- Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, Carragee E, et al. Report of the NIH Task Force on research standards for chronic low back pain. Physical therapy. 2015;95(2):e1-e18.
- Allegri M, Montella S, Salici F, Valente A, Marchesini M, Compagnone C, et al. Mechanisms of low back pain: a guide for diagnosis and therapy. F1000Research. 2016;5.
- Shipton EA. Physical therapy approaches in the treatment of low back pain. Pain and therapy. 2018;7(2):127-37.
- Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, Booth MS, et al. Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. The Spine Journal. 2018;18(5):866-79.
- Haile G, Hailemariam TT, Haile TG. Effectiveness of Ultrasound Therapy on the Management of Chronic Non-Specific Low Back Pain: A Systematic Review. Journal of Pain Research. 2021;14:1251.
- Madson TJ, Hollman JH. Lumbar traction for managing low back pain: a survey of physical therapists in the United States. journal of orthopaedic & sports physical therapy. 2015;45(8):586-95.
- Akhtar MW, Karimi H, Gilani SA. Effectiveness of core stabilization exercises and routine exercise therapy in management of pain in chronic non-specific low back pain: A randomized controlled clinical trial. Pakistan journal of medical sciences. 2017;33(4):1002.
- Wong J, Côté P, Sutton D, Randhawa K, Yu H, Varatharajan S, et al. Clinical practice guidelines for the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. European journal of pain. 2017;21(2):201-16.
- Gordon R, Bloxham S, editors. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. Healthcare; 2016: Multidisciplinary Digital Publishing Institute.
- Searle A, Spink M, Ho A, Chuter V. Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clinical rehabilitation. 2015;29(12):1155-67.
- Vanti C, Andreatta S, Borghi S, Guccione AA, Pillastrini P, Bertozzi L. The effectiveness of walking versus exercise on pain and function in chronic low back pain: a systematic review and meta-analysis of randomized trials. Disability and rehabilitation. 2019;41(6):622-32.
- You JH, Kim S-Y, Oh D-W, Chon S-C. The effect of a novel core stabilization technique on managing patients with chronic low back pain: A randomized, controlled, experimenter-blinded study. Clinical rehabilitation. 2014;28(5):460-9.
- Dineshkumar SK, Dibyendunarayan B, Ramalingam A T. Effect of abdominal drawing-in maneuver along with resisted ankle dorsi-flexion to activate transverse abdominis muscle in chronic non-specific low back pain. Romanian Journal of Physical Therapy/Revista Romana de Kinetoterapie. 2015;21(36).
- Kendall KD, Emery CA, Wiley JP, Ferber R. The effect of the addition of hip strengthening exercises to a lumbopelvic exercise programme for the treatment of non-specific low back pain: A randomized controlled trial. Journal of science and medicine in sport. 2015;18(6):626-31.
- Kim B, Yim J. Core stability and hip exercises improve physical function and activity in patients with non-specific low back pain: A randomized controlled trial. The Tohoku Journal of Experimental Medicine. 2020;251(3):193-206.
- McCaskey MA, Wirth B, Schuster-Amft C, de Bruin ED. Postural sensorimotor training versus sham exercise in physiotherapy of patients with chronic non-specific low back pain: An exploratory randomised controlled trial. PloS one. 2018;13(3):e0193358.
- Nugraha MHS, Antari NKAJ, Dewi AANTN. Differences in the Effectiveness of Proprioceptive Neuromuscular Facilitation Compared with Sensory Motor Training in Non-Specific Low Back Pain. Jurnal Keterapian Fisik. 2021:1-10.
- Brooks C, Kennedy S, Marshall PW. Specific trunk and general exercise elicit similar changes in anticipatory postural adjustments in patients with chronic low back pain: a randomized controlled trial. Spine. 2012;37(25):E1543-E50.
- Gatti R, Faccendini S, Tettamanti A, Barbero M, Balestri A, Calori G. Efficacy of trunk balance exercises for individuals with chronic low back pain: a randomized clinical trial. journal of orthopaedic & sports physical therapy. 2011;41(8):542-52.
- Balthazard P, de Goumoens P, Rivier G, Demeulenaere P, Ballabeni P, Dériaz O. Manual therapy followed by specific active exercises versus a placebo followed by specific active exercises on the improvement of functional disability in patients with chronic non specific low back pain: a randomized controlled trial. BMC musculoskeletal disorders. 2012;13(1):1-11.
- Zangrando F, Piccinini G, Tagliolini C, Marsilli G, Iosa M, Vulpiani MC, et al. The efficacy of a preparatory phase of a touch-based approach in treating chronic low back pain: a randomized controlled trial. Journal of pain research. 2017;10:941.
- Verbrugghe J, Agten A, Stevens S, Hansen D, Demoulin C, Eijnde BO, et al. Exercise intensity matters in chronic nonspecific low back pain rehabilitation. Med Sci Sports Exerc. 2019;51(12):2434-42.
- Verbrugghe J, Agten A, Stevens S, Hansen D, Demoulin C, Eijnde BO, et al. High intensity training to treat chronic nonspecific low back pain: Effectiveness of various exercise modes. Journal of Clinical Medicine. 2020;9(8):2401.
- Michaelson P, Holmberg D, Aasa B, Aasa U. High load lifting exercise and low load motor control exercises as interventions for patients with mechanical low back pain: a randomized controlled trial with 24-month follow-up. Journal of rehabilitation medicine. 2016;48(5):456-63.
- Vincent HK, George SZ, Seay AN, Vincent KR, Hurley RW. Resistance exercise, disability, and pain catastrophizing in obese adults with back pain. Medicine and science in sports and exercise. 2014;46(9):1693.