
Original Article: JRCRS. 2026:14(2): 112-117
9-Urdu Translation of Denver Sacroiliac Joint Questionnaire (DSIJQ) and Its Validity and Reliability in Sacroiliac Joint Dysfunction (SIJD) Patients: A Cross-Sectional Study
Sumbal Salik1, Somia Faisal2, Laila Niaz Khan3, Raheel Munawar 4
1 Physical Therapist, DHQ Hospital, Okara, Pakistan
2 Physical Therapist, The Children’s Hospital, University of Child Health Sciences Lahore, Pakistan
3 Lecturer, Johar Institute of Professional Studies Lahore, Pakistan
4 Physical Therapist, Naseem Akbar Medical Centre, Lahore, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140209
jrcrs-2026140209 Supplement File
ABSTRACT:
Background: Sacroiliac joint dysfunction (SIJD) is a significant contributor of both chronic low back pain and disability. The Denver Sacroiliac Joint Questionnaire (DSIJQ) is a condition-specific tool designed to evaluate severity of symptoms and functional limitations related to SIJD. However, the lack of Urdu version, limited its accessibility for Urdu speaking populations.
Objective: To translate the DSIJQ into an Urdu version and evaluate its reliability and validity among patients with SIJD.
Methodology: The translation of the questionnaire was conducted according to a conventional method of cross-cultural adaptation, which comprises a forward and a backward translation, expert validation, and pilot testing. The Urdu DSIJQ was used to evaluate 110 patients with clinically confirmed SIJD. Psychometric evaluation included content validity (I-CVI and S-CVI/Ave), internal consistency (Cronbach’s alpha), test-retest reliability (intraclass correlation coefficient, ICC), and construct validity through exploratory factor analysis.
Results: The I-CVI ranged between 0.75-0.95 and S-CVI/Ave was 0.85, thus confirming content validity. Internal consistency was strong (Cronbach alpha = 0.858) and test-retest reliability was excellent (average ICC = 0.858). Factor analysis identified two components explaining 71.62% of the total variance.
Conclusion: Strong validity and reliability make the Urdu version of the DSIJQ an appropriate tool for evaluating sacroiliac joint dysfunction in Urdu-speaking communities. It provides a culturally appropriate choice for clinical assessment and research in Pakistani settings.
Keywords: Denver Sacroiliac Joint Questionnaire, ICC, Low Back Pain, Reliability, SIJD, Urdu Translation Disorder, Mental Health, Medical Students, Social Media
Introduction:
Sacroiliac joint dysfunction (SIJD) is a substantial contributor to chronic low back pain (CLBP), accounting for approximately 15–30% of cases.1 The sacroiliac (SI) joint plays an essential role in maintaining pelvic stability and transmitting mechanical loads from the spine to the lower extremities.2 It serves as a shock absorber, assisting in the dissipation of vertical stresses while walking, bending, and lifting.3 Despite being the biggest diarthrodial synovial joint in the human body, the SI joint is susceptible to dysfunction due to its unique structure, which provides both stability and limited mobility.4
SI joint injuries are frequently caused by recurrent micro trauma or axial loading coupled with abrupt rotational forces. Sacroiliac joint dysfunction (SIJD) can lead to pain, reduced mobility, and impaired quality of life.5,6 SIJD occurs more commonly in women than in men, particularly during pregnancy and the postpartum period, due to increase joint mobility.7 The etiologies of SIJ pain are broadly categorized into traumatic (e.g., motor vehicle accidents, falls, lifting injuries) and non-traumatic (e.g., infections, repetitive stress, multiple pregnancies, or inflammatory joint disease).8 Additional risk factors of SIJ pain includes LLD (leg length discrepancy), abnormal gait, scoliosis, pregnancy, obesity, lumbar fusion surgery, strenuous exercise and physical trauma.9
The Denver Sacroiliac Joint Questionnaire (DSIJQ) is a condition-specific tool used to evaluate the severity of symptoms and functional impairments related to SIJD. It consists of ten items, each assessing a different functional domain: Sitting; getting up from a chair; walking; stair climbing; entering and leaving a car; bending, kneeling, or squatting; lifting; work, leisure, sexual, and social activities; sleep; and stability. Each item is rated on a 6-point Likert scale ranging from 0 (no symptoms) to 5 (severe symptoms), yielding a maximum score of 50.10 Higher ratings point to more severe symptoms and more limited functioning. The overall score is converted to a percentage to reflect the severity of functional limitation as: (total score ÷ 50) × 100.11
The DSIJQ, originally developed in English by Dr. Vikas V. Patel and colleagues in the United States, was specifically designed to address the limitations of generic low back pain scales such as the Oswestry Disability Index (ODI). It has demonstrated strong psychometric qualities, such as high internal consistency, responsiveness to change and test-retest reliability.12 The DSIJQ is not yet widely available in other languages, including Urdu, although it has been translated and psychometrically validated in Japanese.13
In Pakistan, where Urdu is the national language and widely spoken across different regions and ethnic groups, the lack of an Urdu version of the DSIJQ presents a substantial barrier to the efficient diagnosis and treatment of SIJD. This limits its application in both clinical and research setting. Therefore, the aim of this study is to translate, culturally adapt, and validate the DSIJQ in Urdu, allowing it to be used by Urdu-speaking patients with SIJD and improving clinical decision-making in Pakistani healthcare settings.
Methodology
This study developed a linguistically and culturally suitable Urdu version of the Denver Sacroiliac Joint Questionnaire (DSIJQ) by using widely recognized cross-cultural adaptation principles as described by Beaton, Bombardier, and Guillemin. To preserve conceptual equivalency and contextual relevance, the translating process was carried out through a series of structured steps, including forward translation, synthesis, backward translation, expert committee review, and pre-testing.
Permission to translate the DSIJQ into Urdu was obtained from the original author. Forward and backward translations were performed by two independent translators; both native Urdu speakers. Translator 1, a clinically trained professional, had access to the materials of the DSIJQ, while Translator 2, an Urdu literature professor with no prior exposure to the scale, produced two independent translations (T1 and T2). An independent reviewer then synthesized both translations (T1 and T2) to compile a reconciled Version 1, ensuring both medical and linguistic accuracy.
Version 1 was then reviewed by a panel of 20 experienced physical therapists, each with more than 5 years of clinical experience. Based on their feedback, Version 2 was developed, including the required modifications to enhance conceptual clarity and clinical relevance. Version 2 was backward translated into English by two blinded bilingual translators, according to the internationally accepted general guidelines. This version was compared with the original English version, and discrepancies were addressed to produce Version 3. Then, a pilot study involving 50 patients from the target population was conducted using Version 3. Based on feedback and performance, the final Urdu version of the DSIJQ was established.
The translation of DSIQ in the Urdu language did not pose significant linguistic or cultural issues. Nonetheless, some of the words and phrases had to be discussed thoroughly so that they could remain conceptually equal and comprehensible to Urdu-speaking respondents. In a case such as the English word sit, which referred to a longer sitting duration, the word was first translated to read as “بیٹھنا“, however, after an evaluation the phrase “زیادہ دیر تک بیٹھ سکتا ہوں” was adopted as it was more functional endurance of sitting instead of any general sitting behavior. Likewise, the phrase bending, kneeling, squatting was translated to “کمر کے بل جھکنا، گھٹنے ٹیکنا، اور بیٹھنا” to communicate the cultural and anatomically relevant behaviors in Urdu.
A contextual adaptation of the phrase “get in and out of the car” to the local language was done as multiple phrases, amongst them “گاڑی میں اندر اور باہر نکلنا” which meant it was clear to the local people many of whom use either public or personal transport on a regular basis. In back translation, effort was made not to lose the original functional context of the item. Other descriptive expressions of pain, like “the inability to walk more than 100 meters” and “use of a cane or crutches” were translated as “میں 100 میٹر سے زیادہ چلنے سے قاصر ہوں” and “مجھے چھڑی یا بیساکھی استعمال کرنی پڑتی ہے” respectively with prior consent to capture accuracy of the quantitative ability restricted and assistive devices usage element in a culturally acceptable mode. The term that was of specific concern here was “sacroiliac joint instability” and it appeared in items like “I always feel as though my sacroiliac joint is loose or out of place.” After consultation with experts a translation of the phrase was suggested as “میرا سیکرولیک جوڑ ہمیشہ ڈھیلا یا جگہ سے باہر محسوس ہوتا ہے” which gives the best idea about joint laxity experienced by the patients without bringing into the scope of the expression any medical terms, and causing a misunderstanding in the reader.
The terms of social life, housework and hobbies were retained as “سماجی زندگی، گھر کا کام، اور مشاغل” respectively, which is a common usage of Urdu. During the adaptation process of Urdu, regional influences of Persian, Arabic and English were taken into consideration to maintain semantic accuracy together with readability. The third reconciled version in Urdu of the DSIJQ was calculated on percent-agreement. The expert review panel revealed a total agreement on linguistic and clinical relevance of all items, based on which the process of cross-cultural adaptation was found sufficient.
A total of 110 participants were recruited at the outpatient department of the DHQ Hospital, Okara. The sample size was calculated through a subject-to-item ratio method used in psychometric research. It is noted that approximately 92% of research used subject-to-item ratio of >2 while 25% had used >20 ratio [22]. In accordance with a commonly recognized ratio of 10 to 1 item, and using a 10-item questionnaire, 100 participants were necessary; thus, 110 participants were utilized to obtain sufficient reliability and internal consistency analysis.14 All the procedures were conducted by the Declaration of Helsinki, and the Ethical Committee of Johar Institute of Professional Studies was used to give approval (Ref No. JIPS/SPT/REC/25-10). Prior to data collection, all participants gave their informed consent.
The inclusion criteria required participants to be adults aged 18-65 years, with CLBP lasting more than three months, and clinically suspected/ diagnosed to have sacroiliac joint dysfunction (SIJD). Diagnosis was based on pain near the posterior superior iliac spine (PSIS) and at least three positive SIJ provocative tests (e.g., FABER, Gaenslen’s, Compression, Distraction, or Thigh Thrust tests). Additionally, participants were required to be proficient in Urdu and able to independently comprehend and complete the questionnaire.15
Exclusion criteria included a history of spinal or SIJ surgery, acute LBP (duration <3 months), or neurological conditions (e.g., cauda equina syndrome, radiculopathy), inflammatory arthritic (e.g., rheumatoid arthritis, ankylosing spondylitis), spinal or pelvic fractures, infections, tumors, or any psychiatric or cognitive disorders that could impair understanding of the questionnaire. Pregnant women were excluded due to the hormonal and biomechanical influences on SIJ stability.15
The psychometric properties of the final Urdu DSIJQ were assessed as follows. The content validity of the final Urdu translation of Denver Sacroiliac Joint Questionnaire (DSIJQ) was evaluated by Waltz and Bausell method. Each item was examined using the relevance and clarity criteria independently, by twenty physical therapy professionals with > 5 years of clinical experience. To determine reliability of the scale, Internal consistency was evaluated using Cronbach’s alpha. Test-retest reliability was assessed using the Intraclass Correlation Coefficient (ICC) with a subset of participants (n=30) at a 7-day interval. The data were evaluated on normality and linearity to determine whether the data were suitable to be subjected to factor analysis. Construct Validity of the scale was explored using Exploratory Factor Analysis (EFA) conducted through Principal Axis Factoring as it highly effective in identifying latent constructs with non-normally distributed clinical data. The Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s Test of Sphericity were used to assess sampling adequacy and factorability.
The statistical analyses were completed through IBM SPSS Statistics v 25. Urdu-translated DSIJQ internal consistency was determined using Cronbach alpha coefficient. Value < 0.70 was considered unsatisfactory; 0.70-0.79 acceptable; 0.80-0.89 good; and ≥0.90 excellent, showing high item-correlation and internal homogeneity. The Intra-class Correlation Coefficient (ICC) was also determined to evaluate the test-retest reliability, based on responses obtained at two time points. It was interpreted that ICC values <0.50 = poor reliability; 0.50-0.74 = moderate; 0.75-0.89 = good; and ≥ 0.90 = excellent. The precision of reliability estimates was supported by a 95 % confidence interval (CI).
Results
The Urdu DSIJQ was finalized and administered to 110 participants with SIJD. Their demographic characteristics are presented in Table 1.
Expert review confirmed strong content validity. Item Content Validity Index (CVI) was between 0.75 to 0.95, and the average scale content-level validity (S-CVI/Ave) was calculated at 0.85, which means there is overall good content validity. The universal agreement (S-CVI/UA) was shown to be 0.80 which indicates a high content validity in the study of all the 10 items. (Table 2).
The Urdu DSIJQ demonstrated strong internal consistency, with a Cronbach’s alpha of 0.858. Test-retest reliability was excellent, with an average measure ICC of 0.858 (95% CI: 0.707–0.934, p < 0.001). The single measure ICC was 0.377 indicating moderate agreement, and the mean inter-item correlation was 0.387 (Table 3). In the case of factor analysis, KMO measure was used to determine sampling adequacy, and the resultant figure was 0.759 that shows good level of adequate sampling to perform exploratory factor analysis. Also, Bartlett Test of Sphericity was significant (p < 0.001), which meant that the data to analyze were appropriate in terms of factor extraction.
Scree plot indicated 2 components with eigenvalue that was more than 1 of 10 items (Fig. 1). As such, these only two components were used in the factor analysis. There is an obvious inflection point following the second factor while factor analysis demonstrated that both of the elements explained a collective 71.62% of the total variance of the entire items.
| Table 1: Demographic characteristics of 110 Patients | ||
| Variables | ||
| Age (Mean ±S.D) | 44.10±11.14 | |
| Gender | Male (%) | 64 (58.2%) |
| Female (%_) | 46 (41.8%) | |
| Affected Side | Right side (%) | 32 (29.1%) |
| Left side (%) | 18 (16.4%) | |
| Bilateral (%) | 60 (54.4%) | |
| Educational Status | Matric (%) | 30 (27.3%) |
| Intermediate (%) | 24 (21.8%) | |
| Graduated (%) | 56 (50.9%) | |
| Table 2. Item-wise Content Validity Index (I-CVI) Ratings for Urdu-DSIJQ | ||||||
| Sr. No. | DSIJQ Item | Agreement (Out of 20) | % Agreement | I-CVI | ||
| 1 | Sitting | 18/20 | 90% | 0.90 | ||
| 2 | Standing | 15/20 | 75% | 0.75 | ||
| 3 | Walking | 15/20 | 75% | 0.75 | ||
| 4 | Stairs | 16/20 | 80% | 0.80 | ||
| 5 | Car entry/exit | 16/20 | 80% | 0.80 | ||
| 6 | Bending/Kneeling/Squatting | 18/20 | 90% | 0.90 | ||
| 7 | Lifting | 18/20 | 90% | 0.90 | ||
| 8 | Work/Household/Social Activities | 17/20 | 85% | 0.85 | ||
| 9 | Sleep | 19/20 | 95% | 0.95 | ||
| 10 | Sacroiliac Joint Stability | 17/20 | 85% | 0.85 | ||
| Table 3: Internal Consistency and Test-retest reliability of 110 SI joint dysfunction patients | ||
| Variable | Values | |
| Chronbach’s alpha | 0.858 | |
| Intra-class correlation | Single Measure | 0.377 |
| Average Measure | 0.858 | |
| Inter-Item Correlation | 0.387 | |
| Kaiser-Meyer Adequacy (KMO) | 0.759 | |
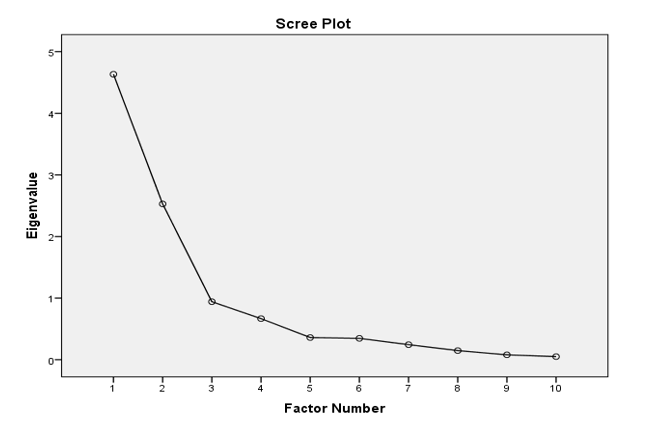
Figure 1: Screen plot showing No. of factors
Discussion
The Urdu version of the Denver sacroiliac joint questionnaire, DSIJQ, was developed according to a standardized, stepwise translation and cultural adaptation process. The translated instrument was psychometrically tested to determine its reliability and validity on the Urdu speaking patients having sacroiliac joint dysfunction (SIJD). The Urdu DSIJQ had 10 items, with a cronbach alpha of 0.858, which is good as an indicator of internal consistency. The test retest reliability indicated a high temporal stability with a mean ICC of 0.858 and a single measure ICC of 0.377. The F-test supported the consistency of repeated measure and proved to be statistically significant (p < 0.001). Expert review confirmed content validity with I-CVI between 0.75 and 0.95 and S-CVI/Ave of 0.85 and S-CVI/UA of 0.80. Factor analysis described construct validity achieving sampling adequacy (KMO value: 0.759), and a significant Bartletts Test (p < 0.001), indicating suitability of the data to extract the factors.
In a pilot study in original English validation conducted by Patel et al. (2023), Denver Sacroiliac Joint Questionnaire (DSIJQ) showed an excellent psychometric outcome, with Cronbach alpha of 0.91 and intraclass correlation coefficient (ICC) of 0.94, reflecting an excellent internal consistency and test retest reliability.12 Similarly, Sawyer et al. (2020) also established that the scale had good reliability and clinical sensitivity to assess SIJ joint dysfunction.16 Comparatively, the internal consistency of the present Urdu version was a bit low (Cronbach alpha less than 0.900/0.858) and the test-retest reliability was moderate (Single 280/Average 796). Such variations can be explained by the factors, including low sample size (n = 110), one-centered data collection focused on Okara, Pakistan, and social linguistic variance of participants.
Similarly, another study translated and redesigned a version of the DSIJQ, as well as verified validity in a sample of patients with SIJD using conservative treatment within Japan. Their results showed that there were Cronbach alpha values greater than 0.85 and ICC of 0.89-0.95, proving about the excellent psychometric strength of the scale. Their exploratory factor analysis as well found a consistently two-factor structure, which was an additional indication of the construct validity of the tool.17 Conversely, Kaiser-Meyer-Olkin (KMO) measure of the present Urdu validation was 0.759 and Bartlett Test of Sphericity was significant (p < 0.001), which reflects appropriate sampling adequacy and fitness to perform factor analysis. In this study, however, the factor structure failed to validate the multi-dimensionality which was reported in other validations potentially because of the low inter-item inter-correlation and small sample size. Such limitations might have limited the mining of discrete underlying details. Nonetheless, the present study is the first to have been adequately translated, culturally adapted, and psychometrically tested of the DSIJQ in the Urdu language. The instrument revealed satisfactory internal consistency and initial structural validity that supported its possible clinical utility to evaluate sacroiliac joint (SIJ) dysfunction in Urdu-speaking communities.
A number of limitations should be taken into consideration. Initially, the research was implemented in one clinical location in Okara; therefore, it can limit the possibility of implementing the results on the broader Pakistani population. Secondly, its relatively small sample size (n = 110) was adequate to carry out explorative analysis but small in respect of more rigorous psychometric data analysis like confirmatory factor analysis. Moreover, unlike the English and Japanese validations, this research was not used in undermining the convergent or criterion-related validity with other existing forms of disability or pain assessment like the Oswestry Disability Index (ODI), Visual Analogue Scale (VAS), or SF-36. The lack of such comparisons restrains the width of construct verification in the Urdu version. These findings were in line with previous research 13, 16 establishing the need to include concurrent measures to conclusively determine the psychometric soundness of the DSIJQ. Finally, the responsiveness of the scale to clinical change was not identified.
Therefore, the future research work must be conducted in multi-centers and different geographical areas to enhance the generalizability of the results. Secondly, it is also important to increase the sample in order to permit the use of confirmatory factor analysis and stronger psychometric tests. Moreover, the use of established instruments like ODI, VAS and SF-36 are to be included to achieve the convergent and criterion validity among the Urdu speaking people. Finally, the test-retest reliability and responsiveness to change overtime should be recommended by longitudinal designs that will enhance the clinical applicability and interpretability of Urdu DSIJQ.
Conclusion
The Urdu translation of the Denver Sacroiliac Joint Questionnaire (DSIJQ) was completed successfully. The Urdu version demonstrated good content validity and adequate reliability when used to evaluate sacroiliac joint dysfunction in Urdu speaking patients.
References
- Vanaclocha V, Jordá-Gómez P, Saiz-Sapena N, Vanaclocha L, Kennedy J. Diagnostic accuracy of clinical examination to distinguish sacroiliac joint pain as a cause of chronic low back pain. British Journal of Neurosurgery. 2024:1-8.
- Waldman LE, Maluli I, Moon CN, Skalski M, Matcuk GR. Sacroiliac joint dysfunction: anatomy, pathophysiology, differential diagnosis, and treatment approaches. Skeletal Radiology. 2024:1-19.
- Newman DP, Soto AT. Sacroiliac joint dysfunction: diagnosis and treatment. American Family Physician. 2022;105(3):239-45.
- Fiani B, Sekhon M, Doan T, Bowers B, Covarrubias C, Barthelmass M, et al. Sacroiliac joint and pelvic dysfunction due to symphysiolysis in postpartum women. Cureus. 2021;13(10).
- Joukar A, Elgafy H, Agarwal AK, Duhon B, Goel VK. The Sacroiliac Joint: A Review of Anatomy, Biomechanics, Diagnosis, and Treatment Including Clinical and Biomechanical Studies (In Vitro and In Silico). Handbook of Spine Technology. 2020:1-26.
- Abdollahi S, Sheikhhoseini R, Rahimi M, Huddleston WE. The sacroiliac dysfunction and pain is associated with history of lower extremity sport related injuries. BMC sports science, medicine and rehabilitation. 2023;15(1):36.
- Ziegeler K, Kreutzinger V, Diekhoff T, Roehle R, Poddubnyy D, Pumberger M, et al. Impact of age, sex, and joint form on degenerative lesions of the sacroiliac joints on CT in the normal population. Scientific Reports. 2021;11(1):5903.
- Waseem A, Manzor N, Fatima I, Yousaf I, Azfar H, Younis H, et al. Comparative effects of mulligan’s mobilization and proprioceptive neuromuscular facilitation technique on pain and disability in patients with sacroiliac joint dysfunction. International Journal of Natural Medicine and Health Sciences. 2023;1(1):1-5.
- Abd-Elsayed A. Sacroiliac Joint Pain: A Comprehensive Guide to Interventional and Surgical Procedures: Oxford University Press; 2021.
- Wessell NM, Wolverton E, Ross P, Akiyama M, Lindley E, Patel V. Opioid prescription monitoring in preoperative and postoperative sacroiliac joint fusion patients. International Journal of Spine Surgery. 2022;16(3):498-504.
- Cleveland Iii AW, Nhan DT, Akiyama M, Kleck CJ, Noshchenko A, Patel VV. Mini-open sacroiliac joint fusion with direct bone grafting and minimally invasive fixation using intraoperative navigation. Journal of Spine Surgery. 2019;5(1):31.
- Patel VV, Sawyer EE, Mintken PE, Michener LA, Cofer CL, Lindley EM. Initial validation of a sacroiliac joint-specific disability questionnaire. Orthopedics. 2023;46(6):345-51.
- Ken Sasaki 1 DK, Eiichi Murakami 2 , Takashi Watanabe 3 , Hiroshi Ei 4. Functional assessment of sacroiliac joint dysfunction using the Denver Sacroiliac Joint Questionnaire. Clinical Journal of Orthopedic Surgery, . 2021;72(10):1076-9.
- Hashemi Zenooz G, Taheriazam A, Mosallanezhad Z, Gabel CP, Melloh M, Mokhtarinia HR. Translation, Cross-Cultural Adaptation, and Validation of the Persian Version of the Harris Hip Score. Arthroplast Today. 2024;27:101384.
- Pervaiz R, Faisal S, Safdar N, Saleem F, Asim HM. Severity of central sensitization in patients with chronic low back pain. Foundation University Journal of Rehabilitation Sciences. 2023;3(2):77-84.
- Sawyer E, Lindley E, Michener L, Patel V, Mintken P, editors. Validation of a new outcome measure for sacroiliac joint pain–The Denver SI Joint Questionnaire (DSIJQ)2020 2020.
- Ken Sasaki DK, and Eiichi Murakami. Functional evaluation of sacroiliac joint dysfunction using the Denver Sacroiliac Joint Questionnaire: A study in the conservative treatment group. Journal of Spine Research. 2022;13(6):875-80.