
Original Article: JRCRS. 2026:14(2): 92-97
6-Assessment of Kinesiophobia in Postoperative Cardiac Patients: A Cross-Sectional Study
Naeem Uddin1, Hayat Ullah2, Sara Alam3, Seema Gul4
1 Managing Director, Dir Rural Development Organization-KP, Pakistan
2 Physical Therapist, Rehab Care Clinic, Peshawar, Pakistan
3 Rehab House Officer, Hayatabad Medical Complex, Peshawar, Pakistan
4 Lecturer, Khyber Medical University, Peshawar, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140206
ABSTRACT:
Background: Cardiac surgeries are commonly and successfully performed to treat various cardiovascular disorders. Postoperative cardiac rehabilitation is essential to minimize the negative effects of surgery. Despite this, cardiac rehabilitation is not routinely practiced in many developing countries. Subsequently, patients often avoid physical activity and exercise due to fear or lack of guidance.
Objective: To evaluate the level of fear of movement and exercise in patients attending cardiac rehabilitation.
Methodology: This was a cross-sectional study conducted on post-operative cardiac patients visiting cardiac rehabilitation department at Peshawar Institute of Cardiology. A total of 277 patients (mean age 50.9±15 years) were recruited in the study through convenience sampling technique. Both male (n= 126) and female (n=91) were included in the study. All the patients were assessed for fear of movement by using Tampa scale for kinesiophobia. Data was analyzed through Statistical Package for the Social Sciences (SPSS).
Results: The results of this study reported that fear of movement was significantly higher in male; majority reporting severe to debilitating kinesiophobia (49.44%). Overall (62.6%) patients reported severe form of fear to movement, (16.4%) reported debilitating kinesiophobia while 38% reported mild fear post-operatively in all phases of outpatient cardiac rehabilitation.
Conclusion: It was established that severe debilitating fear of movement is prevalent across all age groups and phases of cardiac rehabilitation, though these factors did not show a statistically significant association with fear levels. The only statistically significant association observed was between gender and fear; males reporting higher levels of kinesiophobia compared to females.
Keywords: Cardiac rehabilitation, Fear of movement, Kinesiophobia
Introduction:
The prevalence of coronary heart disease and heart failure is increasing steadily. Cardiovascular disease is the leading cause of death (around 17.5 million deaths per year) worldwide.1 In developing countries like Pakistan, self-reported cardiovascular disease is as high as 18% and is expected to rise further due to the increasing prevalence of contributing risk factors such as diabetes, hypertension, physical inactivity and smoking.2 The management of cardiovascular disease, on one hand, includes preventive measures like behavioral and environmental modifications like controlling diabetes, obesity and smoking reducing air pollution and physical inactivity.3 On the other hand extensive literature is available on the diversity and beneficial impact of cardiac surgeries on human health and life expectancy.4 In recent years, some studies suggest better health related outcomes by incorporating cardiac rehabilitation as an integral part of patient treatment regimen both preoperatively and postoperatively.5 Cardiac rehabilitation in a comprehensive approach including patient’s education, psychological treatment, nutrition management, smoking / tobacco cessation and adaptation to work and home environment while maintaining an active life style. These components can collectively reduce mortality rate by 50% in cardiac patients.6 Unfortunately, despite the well-established effectiveness of cardiac rehabilitation in improving clinical outcomes, quality of life, and reducing hospital readmissions, as well as its strong endorsement by major international guidelines such as those from the American Heart Association and the European Society of Cardiology, patient participation rates in CR programs have persistently remained below 50%.7, 8 Studies conducted in Canada and the United States have reported referral rates to cardiac rehabilitation programs as low as 30%, highlighting a critical gap between clinical recommendations and real-world practice. This low referral rate is a major barrier to patient enrollment and reflects systemic issues such as lack of standardized referral protocols, limited provider awareness, and disparities in healthcare access.7 In addition to low referral rates, several patient-level and contextual factors contribute to the underutilization of cardiac rehabilitation.9 Emotional responses such as fear, anxiety, low mood, and lack of motivation can significantly hinder participation.10 Moreover, the level of family support plays a critical role in a patient’s decision to engage in and adhere to rehabilitation programs. Practical barriers such as transportation difficulties, long travel distances, and limited availability of CR facilities further reduce accessibility.11,12
“Kinesiophobia” is limitation of motor activity, recognized as phobic behaviors.13 This fear of movement is often strong, irrational, and doesn’t change easily, even when there’s no real danger.14 Qualitative findings from semi-structured interviews have revealed that patients encounter multiple challenges when attending cardiac rehabilitation. A commonly reported theme was the experience of physical limitations following a cardiac event.15 Symptoms such as persistent shortness of breath, fatigue, and reduced mobility were frequently mentioned.15,16 Additionally, many patients expressed a constant fear of experiencing another cardiac event or sudden cardiac death. This psychological burden has a profound impact on their daily lives, negatively influencing their ability to perform routine activities such as household chores, shopping, and even engaging in light physical exercise.17 These factors contribute to reduced confidence and further hinder participation in rehabilitation programs. 11,18 Some studies have emphasized the importance of observing and listening attentively to patients in order to identify subtle signs of fear or anxiety. This is crucial because many patients may feel hesitant, embarrassed, or unwilling to openly express their fears, particularly in clinical settings where they might feel vulnerable or uncertain.19 Therefore an objective assessment of fear related to movement is mandatory to provide clinicians and rehabilitation therapists with valuable insight into a patient’s level of confidence. This understanding is essential for designing an appropriate rehabilitation program. There is a limited body of research that objectively assesses fear in post-operative cardiac patients.
Methodology
This was a descriptive cross-sectional study; conducted on post-operative cardiac patients visiting cardiac rehabilitation department at the Peshawar Institute of Cardiology. Ethical approval was obtained from the Review Committee of Allied Health Sciences, Khyber Medical University (KMU/Dean/AHS-25/807). The sample size was determined using the Raosoft online sample size calculator. A total of 277 patients were recruited through a convenience sampling technique. Both male and female patients aged 18 years and above were included. Patients who had undergone any type of cardiac surgery were eligible for inclusion. Patients were excluded from the study, despite meeting the inclusion criteria, if any level of physical activity was strictly contraindicated by the cardiothoracic team due to an unstable clinical profile. After meeting the eligibility criteria; written informed consent was obtained from patients for participation in the study and sharing information for publication if needed.
Demographic details were obtained from all the patients. To assess the kinesiophobia objectively. Tampa scale of Kinesiophobia (TSK) was used.20 It is a 17-item questionnaire used to assess fear of movement and injury. The total score on the scale ranges from 17 to 68. As indicated in previous literature, a score of 17 on Tampa indicates no kinesiophobia and a score equal to or above 37 suggests the presence of kinesiophobia.21
Data was analyzed using the Statistical Package for the Social Sciences (SPSS), version 26. Descriptive statistics, including means, standard deviations, and frequency tables, were used to summarize the sample characteristics. The chi-square test and cross-tabulations were conducted to examine the relationship between kinesiophobia and other variables.
Results
The mean age of patients was 50.9 ± 15.5 years. Patients were divided into young, middle aged and senior adults based on their age. In this sample, 66.2% were males and 32.4% were females.
Fear of movement was assessed and scored on Tampa scale. Patients were then divided into 3 categories based on their scoring. Patients scoring 17 were classified as no fear, 18 to 36 as mild fear of movement, scoring 37 to 55 as severe fear and 56 and above were classified debilitating fear. Chi square test was applied to find the impact of different variables degree of fear in post-operative cardiac patients. (see Table2) (Figure 1: a,b,c,d).
| Table 1: Sample Characteristics | ||
| Variable | Categories | (No. of patients; n) (%) |
| Mean Age | Young Adults
(18 to 39) |
n=68 (24.5%) |
| Middle Aged Adults
(40 to 59) |
n=121 (43.6%) | |
| Senior Adults
(60 & above) |
n=88 (31.7%) | |
| Gender | Male | n= 186 (67.1%) |
| Female | n= 91 (32.8%) | |
| Cardiac surgical procedure Type | Coronary Artery Bypass Graph | n=125 (45.1%) |
| Heart valve Replacement /Repair | n=89 (32.1%) | |
| Coronary Angioplasty | n=63 (22.7%) | |
| Post-Discharge Post-operative time period | Phase I
(1 to 3 Months) |
n=89 (32.1%) |
| Phase II
(3 to 6 Months) |
n=74 (26.7%) | |
| Phase III
(6 to 9 Months) |
n=79 (28.5%) | |
| Phase IV
(9 to 12 Months) |
n=35 (12.6%) | |
| Table 2: Correlation of Fear of Movement with Various Determinants | |||||
| Variable | Categories | Mild Fear | Severe Fear | Debilitating Fear | P value |
| Age | Young Adults | 10 (3.6%) | 48 (17.3%) | 10 (3.6%) | P=0.5 |
| Middle aged adults | 29 (10.4%) | 73 (26.3%) | 19 (6.8%) | ||
| Senior adults | 10 (3.6%) | 19 (6.8%) | 17(6.1%) | ||
| Gender | Male | 49 (17.6%) | 104 (37.54%) | 33(11.9%) | P= 0.01 |
| Female | 8(2.8%) | 70(25.2%) | 13 (4.6) | ||
| Cardiac surgical procedure Type | Coronary Artery Bypass Graph | 27(9.7%) | 78(28.1) | 20 (7.2%) | P=0.694 |
| Heart valve Replacement /Repair | 18(6.4%) | 59(21.2%) | 12 (4.3%) | ||
| Coronary Angioplasty | 12(4.3%) | 37 (13.35%) | 14 (5.0%) | ||
| Post-Discharge Post-operative time period | Phase I
(1 to 3 Months) |
22 (7.9%) | 53(19.1%) | 14 (5.0%) | P=0.517 |
| Phase II
(3 to 6 Months) |
18(6.4%) | 43(15.5%) | 13 (4.6%) | ||
| Phase III
(6 to 9 Months) |
12 (4.3%) | 52 (18.7) | 15(5.4%) | ||
| Phase IV
(9 to 12 Months) |
5 (1.8%) | 26(9.3%) | 4(1.4%) | ||
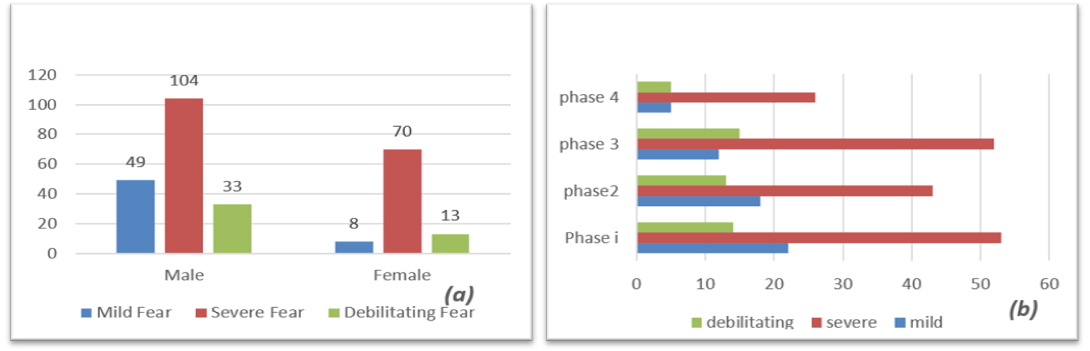
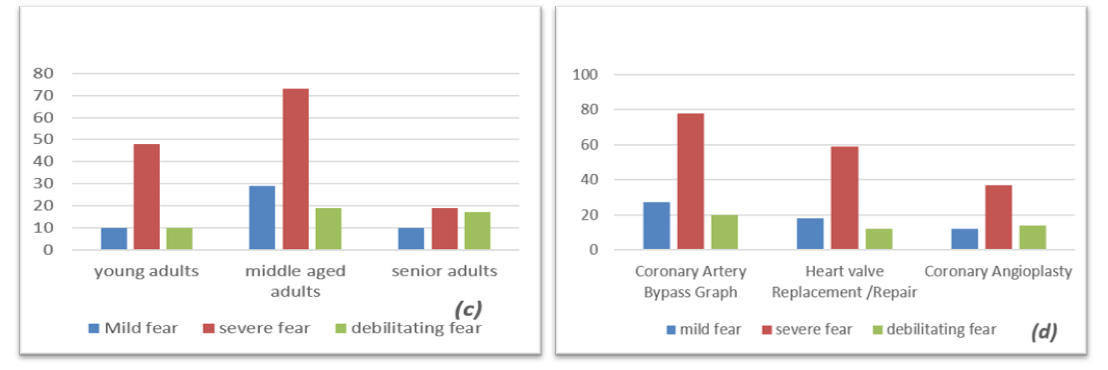
Figure 1: Trends of fear of movement across (a)Gender (b) Different phases of cardiac rehabilitation (c) Different categories of age (d) Types of surgery
Discussion
In this study, we determined that severe debilitating types of kinesiophobia is highly prevalent in patients after cardiac surgery.
We observed that, in our sample, the number of patients who underwent cardiac surgery increased with age. 43.6% were between 40 and 59 years old, and 31.7% were 60 and above years. These findings are consistent with previous literature. As concluded by Kaneko et al., in a cohort of 3027839 patients followed up for 3 years, the incidence of myocardial infarction, angina pectoris, stroke, and heart failure was shown to increase progressively with age.22
The Global Cardiovascular Risk Consortium collected data from 112 individual cohort studies conducted in 34 countries. Based on this study, the examination of 1,518,028 participants followed up for 7.3 years showed that women are slightly at higher risk of developing cardiovascular diseases (57.2%) than males (52.6%).23 A similar study was conducted on global risk factors for heart diseases, by Poulter et al. He concluded that young–middle aged women are relatively at higher risk of developing cardiovascular diseases.24 Contrary to that, our study sample showed a large number of male cardiac patients (67.1%). The lower proportion of females in our study can be associated with multiple factors as determined by Yohannes et al.12, who reported that significant drop in female attendance during cardiac rehabilitation is associated with the lack of adequate family support; women prioritized family responsibilities and time at home over attending rehabilitation sessions. Additionally, limited accessibility to the rehabilitation centers further hindered their participation.12
One of the major findings of our study determines a significant association between gender and fear. The male participants (49.44%) reported higher levels of kinesiophobia compared to females (29.8%). These observations differ from prior literature as determined in a meta-analysis of 15 studies from 6 different countries conducted by Liu L et al. Based on subgroup analysis they revealed that kinesiophobia is not associated with gender; both men and women with cardiovascular conditions experience the same level of fear of movement.25 The heightened levels of kinesiophobia among males in our study could be attributed to certain factors like their involvement in physically demanding occupation. Additionally, males are considered primary economic providers in our culture in contrast to females who are less engaged in informal or physical demanding jobs.
In our study, kinesiophobia was universally present; none of patients reported its absence. 85 % of young adults, 76 % of middle‑aged adults, and 78 % of older adults in our sample reported high levels of kinesiophobia indicating that severe‑to‑debilitating fear of movement is spread across the lifespan. Although these percentages appear slightly different, statistically no significant association between age group and fear intensity can be established. In other words, the likelihood of experiencing pronounced kinesiophobia was similarly high regardless of whether the participant was in the young, middle‑aged, or senior category. In a previously conducted study by Knapik et al. he examined 135 people diagnosed with stable coronary artery disease CAD, age 65 to 88 years (59 females and 76 male). He concluded in his study that movement related fear is more common in elderly population. The reason for these findings can be due to the inclusion of elderly population (age 65 above) while in our study age restrictions were not applied and we observed a high level of movement related fear across all age groups. Clinically, the uniformly high prevalence as shown in our study underscores the need for screening and addressing kinesiophobia in rehabilitation programs for all age brackets, not just older adults who are traditionally viewed as more vulnerable.26
In our study, the level of fear of movement (kinesiophobia) was not found to be statistically associated with the different phases of cardiac rehabilitation. However, a closer look at the distribution revealed that severe debilitating levels of fear were present across all phases: 53% in Phase I, 74% in Phase II, 52% in Phase III, and 85% in Phase IV. This pattern suggests that while the statistical relationship may not be significant, the prevalence of intense fear remains clinically relevant throughout rehabilitation. Notably, the sharp rise in Phase IV may indicate that as patients progress to more advanced stages of rehabilitation, where expectations for physical activity and independence increase, they may experience heightened fear. This could stem from concerns about overexertion, fear of recurrence, or decreased confidence in their physical capabilities, as determined by Nedder et al in a systematic review on psychological impact of anterior cruciate ligament (ACL) reconstruction on rehabilitation. According to his review, patients with ACL reconstruction commonly experience fear of movement as well as fear of re-injury. Lower self-efficacy, higher pain, impaired knee function and poor quality of life were among the major findings of his review.27
Limitation and Recommendation: This was a single-center study, which may limit the generalizability of the findings. Additionally, kinesiophobia was measured by using self-reported TSK, therefore scores may be influenced by reporting or desirability bias. Future studies should incorporate more objective, performance-based assessments alongside validated tools that comprehensively address all components of the biopsychosocial model of fear.
Conclusion
Our study revealed that severe debilitating fear of movement (kinesiophobia) is highly prevalent across all age groups and phases of post-operative cardiac rehabilitation, even though these factors did not show a statistically significant association with fear levels. The only statistically significant association observed was between gender and fear, with male participants reporting higher levels of kinesiophobia compared to females.
References
- Vervoort D, Meuris B, Meyns B, Verbrugghe P. Global cardiac surgery: access to cardiac surgical care around the world. J Thorac Cardiovasc Surg. 2020;159(3):987-96. e6
- Zubair F, Nawaz SK, Nawaz A, Nangyal H, Amjad N, Khan MS. Prevalence of cardiovascular diseases in Punjab, Pakistan: a cross-sectional study. Journal of Public Health. 2018;26(5):523-9.
- Goldsborough E, Osuji N, Blaha MJ. Assessment of cardiovascular disease risk: a 2022 update. Endocrinol Metab Clin North Am. 2022;51(3):483-509.
- Doenst T, Caldonazo T, Schneider U, Moschovas A, Tkebuchava S, Safarov R, Diab M, Färber G, Kirov H. Cardiac surgery 2020 reviewed. Thorac Cardiovasc Surg. 2021.
- Kourek C, Dimopoulos S. Cardiac rehabilitation after cardiac surgery: An important underutilized treatment strategy. World J Cardiol. 2024;16(2):67.
- Zaree A, Dev S, Khan IY, Arain M, Rasool S, Rana MAK, Kanwal K, Bhagat R, Prachi F, Puri P. Cardiac rehabilitation in the modern era: optimizing recovery and reducing recurrence. Cureus. 2023;15(9):e46006.
- Grace SL, Bennett S, Ardern CI, Clark AM. Cardiac rehabilitation series: Canada. Prog Cardiovasc Dis. 2014;56(5):530-5.
- Dalal HM, Doherty P, Taylor RS. Cardiac rehabilitation. Bmj. 2015;351:h5000.
- Khadanga S, Gaalema DE, Savage P, Ades PA. Underutilization of cardiac rehabilitation in women: barriers and solutions. J Cardiopulm Rehabil Prev. 2021;41(4):207-13.
- Chauvet-Gelinier J-C, Bonin B. Stress, anxiety and depression in heart disease patients: A major challenge for cardiac rehabilitation. Ann Phys Rehabil Med 2017;60(1):6-12.
- Campkin LM, Boyd JM, Campbell DJ. Coronary artery disease patient perspectives on exercise participation. J Cardiopulm Rehabil Prev. 2017;37(5):305-14.
- Yohannes AM, Yalfani A, Doherty P, Bundy C. Predictors of drop-out from an outpatient cardiac rehabilitation programme. Clin Rehabil. 2007;21(3):222-9.
- Alpalhao V, Cordeiro N, Pezarat-Correia P. Kinesiophobia and fear avoidance in older adults: a scoping review on the state of research activity. J Aging Phys Act. 2022;30(6):1075-84.
- Goubran M, Farajzadeh A, Lahart IM, Bilodeau M, Boisgontier MP. Kinesiophobia and physical activity: A systematic review and meta-analysis. MedRxiv. 2023:2023.08. 17.23294240.
- McHale S, Astin F, Neubeck L, Dawkes S, Hanson CL. A systematic review and thematic synthesis exploring how a previous experience of physical activity influences engagement with cardiac rehabilitation. Eur J Cardiovasc Nurs. 2020;19(1):31-43.
- Gardner G, Elliott D, Gill J, Griffin M, Crawford M. Patient experiences following cardiothoracic surgery: an interview study. Eur J Cardiovasc Nurs. 2005;4(3):242-50.
- Martens EJ, de Jonge P, Na B, Cohen BE, Lett H, Whooley MA. Scared to death? Generalized anxiety disorder and cardiovascular events in patients with stable coronary heart disease: The Heart and Soul Study. Arch Gen Psychiatry. 2010;67(7):750-8.
- Lee M, Wood T, Chan S, Marziali E, Tang T, Banner D, Lear SA. Cardiac rehabilitation program: an exploration of patient experiences and perspectives on program dropout. Worldviews Evid Based Nurs. 2022;19(1):56-63.
- Bäck M, Caldenius V, Svensson L, Lundberg M. Perceptions of kinesiophobia in relation to physical activity and exercise after myocardial infarction: a qualitative study. Phys Ther. 2020;100(12):2110-9.
- Weermeijer JD, Meulders A. Clinimetrics: Tampa scale for kinesiophobia. J Physiother. 2018;64(2):126.
- Dupuis F, Cherif A, Batcho C, Massé-Alarie H, Roy J-S. The Tampa Scale of Kinesiophobia: a systematic review of its psychometric properties in people with musculoskeletal pain. Clin J Pain. 2023;39(5):236-47.
- Kaneko H, Yano Y, Okada A, Itoh H, Suzuki Y, Yokota I, Morita K, Fujiu K, Michihata N, Jo T. Age‐dependent association between modifiable risk factors and incident cardiovascular disease. J Am Heart Assoc. 2023;12(2):e027684.
- Consortium GCR. Global effect of modifiable risk factors on cardiovascular disease and mortality. N Engl J Med. 2023;389(14):1273-85.
- Poulter N. Global risk of cardiovascular disease. Heart. 2003;89(suppl 2):ii2-ii5.
- Liu L, Yang Q, Li T, Xie H, Zeng B, Zha L, Zhang W, Su S. Prevalence and influencing factors of kinesiophobia in patients with heart disease: a meta-analysis and systematic review. Sci Rep. 2024;14(1):18956.
- Knapik A, Dąbek J, Brzęk A. Kinesiophobia as a problem in adherence to physical activity recommendations in elderly polish patients with coronary artery disease. Patient Prefer Adherence. 2019:2129-35.
- Nedder VJ, Raju AG, Moyal AJ, Calcei JG, Voos JE. Impact of psychological factors on rehabilitation after anterior cruciate ligament reconstruction: a systematic review. Sports Health. 2025;17(2):291-8.