
Original Article: JRCRS. 2026:14(2): 77-84
4-Effects of Scapular Proprioceptive Neuromuscular Facilitation on Pain and Range of Motion in Patients with Adhesive Capsulitis: A Randomized Controlled Trial
Maryum Fatima1, Manahil Shahid2, Sana Bashir3, Haleema Zafar4
1 Student, Foundation University Islamabad, Islamabad, Pakistan
2 Lecturer, Foundation University Islamabad, Islamabad, Pakistan
3 Assistant Professor, Foundation University Islamabad, Islamabad, Pakistan
4 Student, Virtual University of Pakistan, Lahore, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140204
ABSTRACT:
Background: Adhesive capsulitis is a common musculoskeletal condition exhibiting pain and a gradual loss of range of motion in the glenohumeral joint. This affects the activities of daily life and most commonly results in functional limitations.
Objective: To assess the effects of proprioceptive neuromuscular facilitation (PNF) technique on scapula along with conventional physical therapy on pain reduction and improvement in the range of motion of shoulder joints in patients with adhesive capsulitis.
Methodology: At the department of Physical medicine and rehabilitation of Fauji Foundation Hospital, Rawalpindi and District Head Quarter Hospital, Jhelum a single-blind randomized controlled trial was carried out, dated from October 2022 to September 2023. A total of 32 patients with diabetes, aged 40 years and above, both males and females who were diagnosed with pain in one shoulder and whose range of motion was limited were included in this study. Patients with prior shoulder surgery, manipulation under anesthesia, corticosteroid injections within the last three months, or any musculoskeletal, neurological, or cardiovascular disorders were not included in this study. Conventional physiotherapy was given to the control group, and scapular proprioceptive neuromuscular facilitation with conventional treatment was given to the experimental group for two weeks. Pain (visual analogue scale), shoulder ROM (goniometer), and scapular dyskinesia (LSST), were the outcome measures which were assessed at baseline and after two weeks as well. (Clinical Trial Registry Number: NCT05889065)
Results: A total of 32 participants were randomized (n=16 per group). VAS differences between groups were non-significant at baseline (p=0.052) and at 2 weeks (p=0.277), although both groups improved significantly over time (p<0.001). Significant between-group effects were observed for shoulder flexion (168.12 ± 11.08 vs. 146.80 ± 18.51; p=0.001) and abduction (165.62 ± 10.93 vs. 142.80 ± 22.94; p=0.001), but not external rotation (p=0.145). LSST values were comparable at neutral and 45°, with a significant difference at 90° (p=0.031). Within-group improvements were significant at 45° and 90° positions in both groups (p<0.05). The experimental group demonstrated clinically greater improvement across most outcomes.
Conclusion: Scapular PNF combined with conventional physiotherapy produced greater improvements in pain, shoulder range of motion, and selected measures of scapular stability than conventional therapy alone. These findings support the added benefit of incorporating scapular PNF techniques in the rehabilitation of patients with diabetic shoulder dysfunction.
Keywords: Adhesive Capsulitis, Pain, Physical Therapy Modalities, Proprioceptive Neuromuscular Facilitation, Range of Motion, Articular
Introduction:
Frozen shoulder is another name for adhesive capsulitis (AC), is a progressive disorder described by discomfort, stiffness, and functional limitation due to thickening and contracture of the glenohumeral joint capsule.1 First described in the late 19th century and later termed “frozen shoulder,” 2 AC is one of the most prevalent shoulder conditions, affecting 2–5% of the general population and disproportionately impacting females and individuals aged 40–65 years. Its clinical significance is elevated by the association of frozen shoulders with other systemic conditions such as diabetes mellitus, thyroid disorders, and post-immobilization states. This association further elevates its clinical significance.3
According to certain studies, up to 20% of patients with diabetes develop AC, with local data showing prevalence rates exceeding 40% among diabetic individuals. It is a conventional belief that adhesive capsulitis is a self-limiting condition, and it goes away within two to three years. Insite of this belief new research tell that up to 40% of the patients with AC still depict pain, stiffness and impairment in shoulder even after three years. According to the clinical point of view adhesive capsulitis progresses through painful, frozen, and thawing stages, each stage is associated with distinct inflammatory and capsular changes of the joint. Functional impairment is caused by persistent capsular contracture, reduced capsular volume, and altered joint mechanics.4-6
Scapular dyskinesia is a critical yet often overlooked component of AC pathology. It is caused by abnormal scapular motion and positioning due to altered neuromuscular control. Dyskinesia disrupts the scapulohumeral rhythm, increases mechanical stress on surrounding tissues, and causes pain, restricted range of motion, and reduced response to treatment. Impingement syndromes, rotator cuff pathology, and glenoid labral injuries are commonly reported in AC.7
Adhesive capsulitis can be primary (idiopathic) or secondary to systemic diseases, shoulder trauma, or surgery. Patients typically complain of night pain, progressive stiffness, and significant loss of external rotation and abduction. Functional loss is caused by capsular inflammation, fibrosis, adhesion of the axillary recess, and diminished proprioception.8 Individuals aged from 40 to 65 years often have this disorder and it makes them fall into the category of three to five percent of the overall population having this disorder. Ten to thirty eight percent of the patients have thyroid related problems and diabetes mellitus.9 Adhesive capsulitis most commonly start in the 50s and 60s, although the highest prevalence of this disease is in the middle of the 50s.10
Pharmacological interventions, intra-articular corticosteroid injections, and physical therapy (PT) are the interventions which are used to treat this disease. Physical therapy is primarily used to treat adhesive capsulitis, particularly in the painful and frozen stages. Thermotherapy, Ultrasound, TENS, joint mobilizations, stretching, and active and passive range-of-motion exercises are the common interventions. According to the evidence structured rehabilitation improves pain, range of motion, and function; however, recovery is limited due to long-term immobilization which most commonly results into secondary scapular dyskinesia.11
In the early stage the treatment plan emphasizes patient education, pain management, and to control and decrease inflammation. Physical therapy and non-steroidal anti-inflammatory medications (NSAIDs) are most recommended in early stages.12 Neuromuscular activation, proprioception, and coordinated movement through targeted diagonal movement patterns and facilitated stretching are enhanced by proprioceptive neuromuscular facilitation (PNF) techniques. Scapula plays an important role in the biomechanics of upper limb, and impaired scapular control can have negative impact on glenohumeral rehabilitation. Scapular Proprioceptive Neuromuscular Facilitation techniques such as anterior elevation and posterior depression patterns, repeated stretch, and hold-relax methods facilitate muscle activation, improving scapular stability, and restore optimal movement patterns.13
Even though conventional physical therapy interventions are used in the management of adhesive capsulitis, most interventions most importantly focus on the glenohumeral joint, targeting on capsular stretching, joint mobilization, and restoration of passive and active range of motion. Scapulothoracic joint plays a vital role in the maintenance of normal and coordinated function of shoulder and normal scapulohumeral rhythm but the above-mentioned interventions often do not focus on the scapulothoracic joint, but the capsular restrictions are effectively managed through these interventions. According to the available evidence, pain, restricted range of motion, and functional impairment are also caused by scapular dyskinesia in adhesive capsulitis. Proprioceptive neuromuscular facilitation (PNF) aims to improve neuromuscular control, contributes in the enhancement of proprioception and it also restores the dynamic stability of scapula whereas the interventions which solely focus on glenohumeral joints cannot contribute to the improvement of these factors. Despite this, scapular PNF techniques are not routinely incorporated into conventional rehabilitation protocols, and there is limited evidence specifically evaluating their additive effect in patients with adhesive capsulitis.
Hence, the objective of this study is to investigate the effects of scapular proprioceptive neuromuscular facilitation along with the conventional physical therapy which focuses on glenohumeral joint, to determine whether addressing both components can lead to superior improvements in pain and shoulder range of motion.
Methodology
It was a parallel group, single-blinded randomized controlled trial in which outcome assessors were blinded to group allocation to minimize the biasing of measurements. At the Physical Medicine and Rehabilitation department, Fauji Foundation Hospital Rawalpindi and District Head Hospital Jhelum a randomized controlled trial was conducted, dated from September 2022 to August 2023. Thirty-two participants aged 40 years or older with unilateral stage II or III adhesive capsulitis participated. Patients with prior shoulder surgery or manipulation under anesthesia, corticosteroid injections within the last three months, or any musculoskeletal, neurological, or cardiovascular disorder were not included. Participants were randomized into experimental and control groups using a sealed envelope method, ensuring unbiased allocation. Randomization allowed the study to maintain the precision of the methodology although participants were recruited through non-probability-based purposive sampling. Harvard Sample Size Calculator at a 95% confidence interval was used to calculate the sample size assuming a large effect size (Cohen’s d = 1.0) based on the randomized controlled trials published previously in adhesive capsulitis and shoulder rehabilitation reporting substantial improvements in range of motion of shoulder joint (particularly flexion and abduction) following the interventions of physiotherapy.14 The assumed effect size reflects clinically meaningful gains in ROM observed in these studies, with a power of 80% and alpha of 0.05, resulting in 16 participants per group. The experimental group received scapular proprioceptive neuromuscular facilitation (PNF) in combination with conventional physiotherapy, including diagonal scapular patterns (anterior elevation/posterior depression and posterior elevation/anterior depression) using rhythmic initiation and repeated contractions, for 40 minutes per session, five sessions per week for two weeks. The control group received conventional physiotherapy alone, consisting of shoulder range of motion exercises, stretching, and joint mobilizations (Maitland grades I–II and glenohumeral distraction with caudal, dorsal, and ventral glides) for the same duration and frequency. The intensity of pain which was measured using the Visual Analog Scale (VAS, ICC = 0.99),15 and range of motion (flexion, abduction, and external rotation) which was assessed with a goniometer (ICC > 0.94) were the primary outcomes.16 Scapular mobility which was evaluated using the Lateral Scapular Slide Test (LSST) with vernier calipers was the secondary outcome.17 The participants demographic data was collected via a structured questionnaire. Baseline assessments were performed before randomization, along with post-intervention measurements which were conducted after two weeks using the same tools.
Ethical approval was obtained from the Ethical Review Committee and Institutional Research Committee of Foundation University, Islamabad (FF/FUMC/215-273 Phy/23 & FF/FUCP/934-2/MPTF2110). All participants provided written informed consent before getting enrolled in the study.
SPSS version 21 was used to analyze the data. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as mean ± standard deviation or median with interquartile range, depending on distribution. Normality was assessed by using the Shapiro-Wilk test. Parametric tests (independent t-test for between-group comparisons and paired t-test for within-group comparisons) were used to analyze the variables which met normality assumptions. Whereas non-parametric tests (Mann–Whitney U test for between-group and Wilcoxon Signed-Rank test for within-group comparisons) were used to analyze non-normally distributed variables. Consistency was ensured between normality results, choice of statistical tests, and data presentation via this approach.
No formal correction for multiple comparisons like Bonferroni adjustment, was applied given the exploration nature of the study and the limited sample size. Instead, results were interpreted cautiously, with emphasis placed on consistency across related outcome measures and clinical relevance rather than isolated statistical significance.
Initially, a mixed model (ANOVA/ACNOVA) was considered. However, it was replaced by simpler parametric and non-parametric tests, considering the small sample size, limited repeated time points, as well as the primary goal of comparing pre-post changes among two independent groups. Baseline comparability between groups was confirmed prior to analysis, and change scores were interpreted accordingly to minimize bias. This approach is consistent with previously published randomized controlled trials in adhesive capsulitis with short follow-up durations.
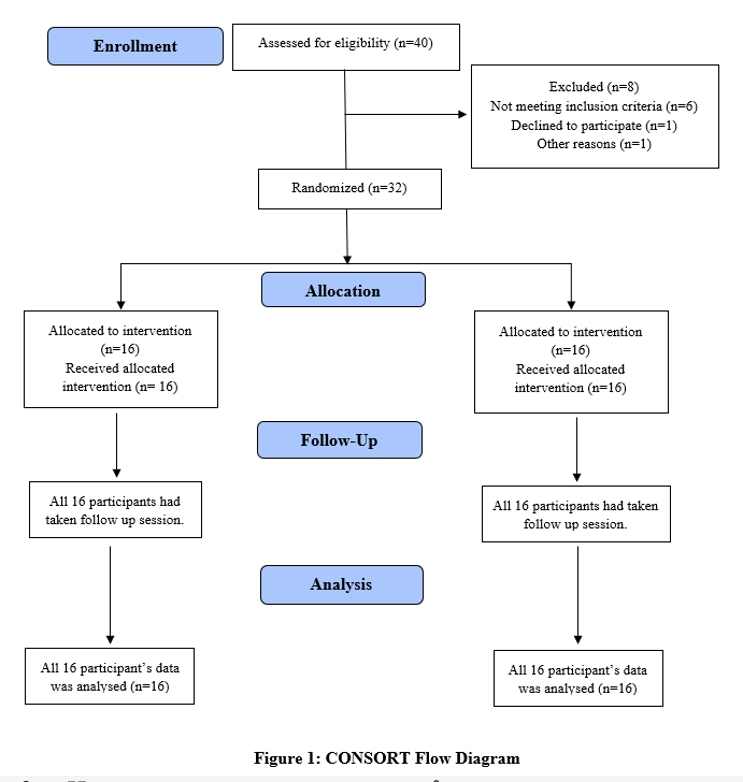
Figure 1: CONSORT Flow Diagram
| Table 1: Normality Analysis | ||||
| Variable | Assessment Point | Experimental (p-value) | Control
(p-value) |
Normality |
| VAS | Baseline | 0.017 | 0.044 | Not normal |
| After 2 weeks | 0.039 | 0.185 | Normal | |
| Flexion | Baseline | 0.043 | 0.086 | Normal |
| After 2 weeks | 0.010 | 0.038 | Not normal | |
| Abduction | Baseline | 0.194 | 0.089 | Normal |
| After 2 weeks | 0.038 | 0.003 | Not normal | |
| External Rotation | Baseline | 0.313 | 0.006 | Not normal |
| After 2 weeks | 0.225 | 0.080 | Normal | |
| LSST Neutral | Baseline | 0.020 | 0.036 | Not normal |
| After 2 weeks | 0.200 | 0.014 | Not normal | |
| LSST 45° | Baseline | 0.248 | 0.049 | Normal |
| After 2 weeks | 0.349 | 0.014 | Not normal | |
| LSST 90° | Baseline | 0.002 | 0.148 | Normal |
| After 2 weeks | 0.020 | 0.680 | Normal | |
| Note: p > 0.05=normally distributed, p < 0.05=non-normally distributed. | ||||
Results
The study included 32 participants with a mean age of 51.03 ± 7.07 years. Of these, 10 (31%) were males and 22 (69%) were females. Regarding hand dominance, 7 participants (21.9%) were left-hand dominant, while 25 (78.1%) were right-hand dominant. Based on clinical classification, 21 individuals (65.6%) had primary disease, whereas 11 (34.4%) had secondary disease. In terms of disease stage, 19 participants (59.4%) were in the frozen stage and 13 (40.6%) were in the thawing stage. The involved side was evenly distributed, with 16 cases (50%) affecting the left shoulder and 16 (50%) affecting the right shoulder shown in Table 2.
Pain (VAS) Scores, Shoulder Range of Motion, and Lateral Scapular Slide Test (LSST) – Within and Between Group Analysis:
Pain (VAS) Scores: Both experimental and control groups showed significant within-group reductions in pain over two weeks (p<0.001). Between-group differences were not statistically significant (p=0.277), although the experimental group demonstrated greater improvement.
Shoulder Range of Motion: Both groups exhibited significant within-group improvements in shoulder flexion and abduction (p<0.05), with the experimental group demonstrating greater gains. External rotation improved significantly only in the control group, with no statistically significant between-group differences.
Lateral Scapular Slide Test (LSST): Within-group analysis showed significant improvements at LSST 45° and 90° in both groups, while LSST neutral did not change significantly. A significant difference at LSST 90° was observed via the between-group analysis. This suggests that at 90°, greater improvement in scapular positioning is observed.
| Table 2: Demographics | |
| Variable | Value (n=32) |
| Continuous Variables | |
| Age (Mean ± SD) | 51.03 ± 7.07 |
| Categorical Variables | |
| Gender | Male: 10 (31%)
Female: 22 (69%) |
| Dominant Hand | Left: 7 (21.9%)
Right: 25 (78.1%) |
| Classification | Primary: 21 (65.6%)
Secondary: 11 (34.4%) |
| Stage of Disease | Frozen: 19 (59.4%)
Thawing: 13 (40.6%) |
| Involved Side | Left: 16 (50%)
Right: 16 (50%) |
Values are presented as mean ± standard deviation for normally distributed data, and as median [interquartile range] for non-normally distributed data. Wilcoxon Signed-Rank test or paired t-test was used for the within-group comparisons. Between-group comparisons were performed using the Mann–Whitney U test or independent t-test.
VAS = Visual Analog Scale;
LSST = Lateral Scapular Slide Test, SD: Standard Deviation
p < 0.05=statistically significant, p > 0.05=statistically non-significant.
Effect size analysis demonstrated very large effects for shoulder flexion (d = 1.39) and abduction (d = 1.28), indicating a strong clinical advantage of scapular proprioceptive neuromuscular facilitation combined with conventional therapy. Moderate effects were observed for pain reduction and external rotation (d = 0.56). Scapular mobility outcomes demonstrated small-to-large effects across different LSST positions (d = 0.45–0.82), reflecting position-specific improvements in scapular control.
| Table 3: Pain (VAS) Scores, Shoulder Range of Motion, and Lateral Scapular Slide Test (LSST) – Within and Between Group Analysis | |||||
| Variable | Group | Baseline Median (IQR) or Mean ±SD | Post 2 Weeks Median (IQR) or Mean ±SD | Within-Group (p-value) | Between-Group (p-value) |
| Pain (Score) | Experimental | 8 (1) | 1 (1.8) | <0.001 | 0.277 |
| Control | 6 (2.8) | 2 (2) | <0.001 | 0.277 | |
|
Shoulder Flexion (°) |
Experimental | 101.25 ± 13.22 | 168.13 ± 11.08 | <0.001 | 0.001 |
| Control | 97.5 ± 31.98 | 146.8 ± 18.51 | 0.002 | 0.001 | |
|
Shoulder Abduction (°) |
Experimental | 100.31 ± 20.69 | 165.62 ± 10.93 | 0.001 | 0.001 |
| Control | 84.37 ± 20.69 | 142.8 ± 22.94 | 0.015 | 0.001 | |
| Shoulder External Rotation (°) | Experimental | 46 ± 9.23 | 77.18 ± 8.36 | 0.975 | 0.145 |
| Control | 45.93 ± 12.67 | 72.18 ± 9.48 | <0.001 | 0.145 | |
| LSST Neutral (cm) | Experimental | 1.275 ± 0.19 | 1.18 ± 0.19 | 0.220 | 0.280 |
| Control | 1.18 ± 0.19 | 1.07 ± 0.29 | 0.245 | 0.280 | |
| LSST 45° (cm) | Experimental | 0.83 ± 0.26 | 0.84 ± 0.45 | <0.001 | 0.777 |
| Control | 0.84 ± 0.45 | 1.14 ± 0.48 | 0.021 | 0.777 | |
| LSST 90° (cm) | Experimental | 1.41 ± 0.40 | 1.17 ± 0.69 | 0.009 | 0.031 |
| Control | 1.17 ± 0.69 | 1.38 ± 0.24 | 0.001 | 0.031 | |
| Table 4: Between-group effect sizes (Cohen’s d) for post-intervention outcomes | |
| Variables | Cohen’s d |
| Pain (VAS) | 0.56 |
| Flexion | 1.39 |
| Abduction | 1.28 |
| External Rotation | 0.56 |
| LSST Neutral | 0.45 |
| LSST 45° | 0.70 |
| LSST 90° | 0.82 |
Discussion
This study examined the short-term (2-week) effects of adding scapular proprioceptive neuromuscular facilitation (PNF) to conventional physical therapy on pain, shoulder range of motion (ROM), and scapular mobility in patients with stage II–III adhesive capsulitis. Over the 2-week intervention period, both groups demonstrated significant within-group reductions in pain, supporting the effectiveness of conventional physiotherapy in alleviating pain during the early phase of rehabilitation. Although pain scores were greatly diminished in the experimental group, the statistical significance was not reached by the between group difference, which shows that there was not much additional analgesic effect of scapular PNF over this short duration. These findings are consistent with Nilay Comuk Balcı et al. (2016), who reported pain reduction following scapular PNF but observed modest between-group differences.8 A significant reduction in pain with PNF-based interventions over short treatment periods, was demonstrated by Mubarka Saeed et al. (2022) but depending on comparator interventions the magnitude of between group differences were varied.20
In the experimental group pain outcomes, shoulder flexion and abduction showed significantly greater improvements as compared to the control group after 2 weeks, with statistically significant between-group differences (p = 0.001). These findings suggest that the scapulothoracic coordination was facilitated and neuromuscular control was improved during overhead motion due to the addition of scapular PNF. This is like the findings by Mahendran et al., who reported that when PNF techniques were combined with conventional therapy compared to conventional therapy alone then there were superior improvements in range of motion.21 The improved flexion and abduction over a short timeframe suggest that scapular-focused facilitation may be much beneficial for movements requiring coordinated scapular upward rotation.
A significant between-group difference was not demonstrated by shoulder external rotation, and improvement was observed only within the control group. This tells that a meaningful change in rotational range of motion cannot be achieved by short term interventions, which is often more restricted in adhesive capsulitis due to capsular tightness. Fredriksen et al., supports this interpretation who found that over 8 weeks additional external-rotation exercises over did not yield superior between-group improvements compared to usual care, strengthening the belief that longer or more targeted interventions are required for rotational gains.22
With respect to scapular positioning, assessment using the Lateral Scapular Slide Test (LSST) demonstrated significant within-group changes at 45° and 90° of abduction, while neutral position measurements remained unchanged. Importantly, a significant between-group difference was observed at 90° abduction, favoring the experimental group (p = 0.031). This finding suggests that scapular PNF may produce early improvements in scapular control at higher degrees of arm elevation, where scapular mechanics are most challenged. Similar observations were reported by Nilay Comuk Balcı et al., who noted subtle but functionally relevant changes in scapular positioning following PNF-based interventions.8 Studies by Tang et al. and Mahmoud et al. further support this interpretation, demonstrating that scapular-specific exercises lead to greater improvements in LSST measurements, particularly at higher abduction angles, compared to conventional exercises alone.23,24
All participants with diabetes mellitus were included in the study, diabetic individuals are known to have more severe and persistent forms of adhesive capsulitis due to underlying connective tissue and metabolic alterations. Advanced glycation end-products (AGEs) are formed due to chronic hyperglycemia, which induce collagen cross-linking and reduced tissue elasticity, which leads to capsular stiffness and restriction in the mobility of shoulder.25 Additionally, chronic low-grade inflammation characterized by elevated cytokines such as interleukin-1 and tumor necrosis factor-alpha is also associated with diabetes which further promotes fibroblast activity and excessive collagen deposition within the joint capsule.26 Microvascular complications and reduced tissue perfusion may further impair tissue repair mechanisms, and the progression of disease is prolonged due to microvascular complications.27
Furthermore, proprioceptive impairments secondary to peripheral neuropathy, are also demonstrated by the diabetic patients which can negatively affect joint position sense and neuromuscular control, thereby scapular mechanics are altered, and it also results in functional limitation of the shoulder complex.
According to the pathological context, in the experimental group there were greater improvements in shoulder elevation and scapular positioning which can be explained by the role of scapular proprioceptive neuromuscular facilitation (PNF) techniques in enhancing neuromuscular activation and proprioceptive input. However, the limited between-group difference in pain reduction may reflect the persistent inflammatory and biochemical milieu associated with diabetes, which may not be fully changeable via short-term rehabilitation alone.
Overall, the findings of this study depict that scapular proprioceptive neuromuscular facilitation (PNF), when added to conventional glenohumeral-focused therapy, enhances short-term improvements in shoulder elevation range of motion and scapular positioning in patients with adhesive capsulitis. No significant between-group difference was observed while both interventions were effective in pain reduction, suggesting that pain modulation may be affected by factors beyond short-term neuromuscular interventions in patients with diabetes. The greater improvements observed in shoulder elevation and scapular control were greatly improved, which highlights the significance of incorporating scapular-focused rehabilitation strategies to address changes in scapulothoracic mechanics and neuromuscular deficits. It is suggested that longer intervention durations may be required to achieve comprehensive functional recovery in diabetic adhesive capsulitis due to limited changes in external rotation.
Conclusion
The addition of scapular proprioceptive neuromuscular facilitation (PNF) to conventional physical therapy resulted in significant improvements in shoulder flexion, abduction, and scapular positioning at higher degrees of abduction in patients with stage two and three adhesive capsulitis. Pain was reduced because of both treatment approaches; however, no significant difference between groups was observed in the reduction of pain. These findings suggest that when incorporated into conventional rehabilitation programs scapular PNF may enhance short-term gains in shoulder elevation movements and scapular control. This study has several limitations. The generalizability of the findings may be limited due to small sample size. Selection bias may be introduced despite random allocation to intervention groups due to the employment of purposive sampling. The intervention and follow-up period were limited to two weeks; hence, the findings depict short-term effects only, and long-term outcomes could not be assessed. Lateral Scapular Slide Test was used to evaluate the scapular positioning, which, although clinically feasible, may not fully capture dynamic scapular motion during functional activities. Future studies with larger sample sizes, longer intervention durations, and extended follow-up periods are recommended to further validate these findings.
References
- Nakandala P, Nanayakkara I, Wadugodapitiya S, Gawarammana I. The efficacy of physiotherapy interventions in the treatment of adhesive capsulitis: A systematic review. Journal of back and musculoskeletal rehabilitation. 2021;34(2):195-205.
- Taha HKA, Mohammed HJ. Journal of Population Therapeutics & Clinical Pharmacology.
- Funk L, Monga P, Walton M. Structural disorders of the shoulder. Oxford Textbook of Musculoskeletal Medicine. 2015:330.
- Kelley MJ, Shaffer MA, Kuhn JE, Michener LA, Seitz AL, Uhl TL, et al. Shoulder pain and mobility deficits: adhesive capsulitis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the Orthopaedic Section of the American Physical Therapy Association. Journal of orthopaedic & sports physical therapy. 2013;43(5):A1-A31.
- Clement R, Ray AG, DaviDson C, Robinson CM, PERks FJ. Frozen shoulder: long-term outcome following arthrographic distension. Acta Orthop Belg. 2013;79(4):368-74.
- DeStefano S, Oberle L, Donohoe B, Kobayashi Y, Gottschalk AW. Optimizing Pain Control and Function in Patients With Adhesive Capsulitis by Choosing the Best Injection Site. The Ochsner Journal. 2022;22(2):107.
- Giuseppe LU, Laura RA, Berton A, Candela V, Massaroni C, Carnevale A, et al. Scapular dyskinesis: from basic science to ultimate treatment. International journal of environmental research and public health. 2020;17(8):2974.
- Balcı NC, Yuruk ZO, Zeybek A, Gulsen M, Tekindal MA. Acute effect of scapular proprioceptive neuromuscular facilitation (PNF) techniques and classic exercises in adhesive capsulitis: a randomized controlled trial. Journal of physical therapy science. 2016;28(4):1219-27.
- Zreik NH, Malik RA, Charalambous CP. Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles, ligaments and tendons journal. 2016;6(1):26.
- Wang K, Ho V, Hunter-Smith DJ, Beh PS, Smith KM, Weber AB. Risk factors in idiopathic adhesive capsulitis: a case control study. Journal of shoulder and elbow surgery. 2013;22(7):e24-e9.
- Ramirez J. Adhesive capsulitis: diagnosis and management. American family physician. 2019;99(5):297-300.
- D’Orsi GM, Via AG, Frizziero A, Oliva F. Treatment of adhesive capsulitis: a review. Muscles, ligaments and tendons journal. 2012;2(2):70.
- Griggs SM, Ahn A, Green A. Idiopathic adhesive capsulitis: a prospective functional outcome study of nonoperative treatment. JBJS. 2000;82(10):1398.
- Henricus M Vermeulen, Piet M Rozing, Wim R Obermann, Saskia le Cessie, Thea PM Vliet Vlieland, Comparison of High-Grade and Low-Grade Mobilization Techniques in the Management of Adhesive Capsulitis of the Shoulder: Randomized Controlled Trial, Physical Therapy, Volume 86, Issue 3, 1 March 2006, Pages 355–368, https://doi.org/10.1093/ptj/86.3.355
- Begum MR, Hossain MA. Validity and reliability of visual analogue scale (VAS) for pain measurement. Journal of Medical Case Reports and Reviews. 2019;2(11).
- Correll S, Field J, Hutchinson H, Mickevicius G, Fitzsimmons A, Smoot B. Reliability and validity of the halo digital goniometer for shoulder range of motion in healthy subjects. International journal of sports physical therapy. 2018;13(4):707.
- Shadmehr A, Sarafraz H, Blooki MH, Jalaie S, Morais N. Reliability, agreement, and diagnostic accuracy of the Modified Lateral Scapular Slide test. Manual therapy. 2016;24:18-24.
- Mena-del Horno S, Dueñas L, Lluch E, Louw A, Luque-Suarez A, Mertens MG, et al. A central nervous system focused treatment program for people with frozen shoulder: a feasibility study. International Journal of Environmental Research and Public Health. 2022;19(5):2628.
- Edwards O, Counihan M, Li X. Epidemiology of frozen shoulder. Frozen Shoulder: Elsevier; 2024. p. 53-7.
- Saeed M, Hafeez S, Asad F, Haider W, Nawaz S, Kocub S. Comparison of scapular proprioceptive neuromuscular facilitation and myofascial release techniques on pain and function in scapular dyskinesia associated with adhesive capsulitis: Scapular dyskinesia associated with adhesive capsulitis. Pakistan BioMedical Journal. 2022:123-7.
- Chetia D. Combined Effects of Joint Mobilization with Proprioceptive Neuromuscular Facilitation in Subjects with Adhesive Capsulitis of Shoulder: Rajiv Gandhi University of Health Sciences (India); 2013.
- Fredriksen H, Cools A, Myklebust G. No added benefit of 8 Weeks of shoulder external rotation strength training for youth handball players over usual handball training alone: a randomized controlled trial. journal of orthopaedic & sports physical therapy. 2021;51(4):174-87.
- Tang L, Chen K, Huang L, Liang J, Wang M, He L, et al. Efficacy of targeted scapular stabilization exercise versus conventional exercise for patients with shoulder pain: a randomized clinical trial. American Journal of Physical Medicine & Rehabilitation. 2024;103(9):771-6.
- Mahmoud LA, Abdulmajeed SF, Abd El-Moneim Ali MA, Mohamed NAA. Effect of Adding Scapular Focused Exercises Program to the Conventional Physical Therapy Program on Shoulder Impingement Syndrome. Egyptian Reviews for Medical and Health Sciences. 2025;4(1):13-32.
- Hernigou P, Scarlat MM. The diabetic shoulder: association between diabetes mellitus and adhesive capsulitis – a systematic review and meta-analysis. Int Orthop. 2026 Apr;50(4):839-851. doi: 10.1007/s00264-026-06793-4. Epub 2026 Mar 28. PMID: 41896299; PMCID: PMC13079542.
- Zreik NH, Malik RA, Charalambous CP. Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles Ligaments Tendons J. 2016 May 19;6(1):26-34. doi: 10.11138/mltj/2016.6.1.026. PMID: 27331029; PMCID: PMC4915459.
- Dimitri-Pinheiro S, Pinto BS, Pimenta M, et al. Influence of diabetes on response to ultrasound-guided hydrodistension treatment of adhesive capsulitis: a retrospective study. BMC Endocr Disord. 2022;22:227.