
Original Article: JRCRS. 2026:14(1):23-28
5-Relationship of Kinesophobia with Pain Intensity, Disability, and Sleep Quality in Patients with Chronic Low Back Pain: A Cross-Sectional Study
Fatima Bibi1, Ayesha Jamil2 Kanwal Arshad3
1 Student, University Institute of Physical Therapy, Faculty of Allied Health Sciences, The University of Lahore, Lahore, Pakistan
2 3 Assistant Professor, University Institute of Physical Therapy, Faculty of Allied Health Sciences, The University of Lahore, Lahore, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140105
ABSTRACT:
Background: Chronic low back pain is one of the major health care concerns. It impacts the activities of daily living and mental well-being. Kinesiophobia is often associated with chronic pain that may lead to a cascade of further movement dysfunctions.
Objective: To explore the relationship of kinesiophobia with pain intensity, disability, and sleep quality in patients with chronic low back pain.
Methodology: The study was conducted at the University of Lahore, and data were collected from the medical and outpatient physiotherapy departments of the University Teaching Hospital, Lahore. A sample of 97 participants was recruited using a convenience sampling technique. The participants of both genders, aged between 18 and 60 years, presenting with chronic low back pain for the last three months, were included. Kinesiophobia. Pain intensity, functional disability, and sleep quality were outcome measures. Spearman’s correlation was used to find the strength and direction of the relationship between variables.
Results: The mean age of participants was 37.38 ±7.045. There were 50 (51.5%) females, and the mean BMI was 22.17 ±1.73 kg/m2. The mean of pain intensity was 6.60±1.04, functional disability was35.84±4.85, sleep quality was 9.52±2.22, and kinesiophobia was 41.20±4.38. The analysis showed a significant positive correlation of kinesiophobia with pain intensity (r=0.294, p=0.003), functional disability (r=0.293, p=0.004), and sleep quality (r=0.426, p=0.001).
Conclusion: Kinesiophobia has a positive relationship with pain intensity, functional disability, and quality of sleep. The higher the level of kinesiophobia, the higher the severity of pain, functional disability, and the poorer the sleep quality.
Keywords: Chronic Low Back Pain, Kinesiophobia, Pain Intensity, Functional Disability, Sleep Quality.
Introduction:
Low back pain is one of the most common musculoskeletal conditions, affecting a significant portion of the global population. According to research, about 39% of people in the general population experience low back pain at some point in their lives, 38% had it in the last 12 months, and 31% had suffered in the previous 30 days. Its prevalence increases with age, with peak incidence around 45-54 years of age, and is common in both genders.1 However, females may have a greater tendency to develop it due to various physical, biomechanical, and hormonal influences.2 If LBP lasts for more than twelve weeks from the onset, then it is labelled as chronic low back pain (CLBP). Being one of the main causes of disability in a variety of age groups, CLBP has a significant worldwide burden that carries high personal and social costs.3 It is estimated that 73.3% of people with chronic LBP experience depression.4
The lumbar spine is made up of complex musculoskeletal systems, including vertebrae, intervertebral discs, ligaments, muscles, and nerves that may be affected in nonspecific low back pain. CLBP is located between the inferior gluteal folds and the costal margins, and frequently results from tension or failure in these physical structures that may be accompanied by radiating pain 5 that has a major impact on everyday functional activities and posture management because this area is essential for trunk stability and mobility.6
CLBP is frequently nonspecific, which means it cannot be linked to a recognized, established pathology like cancer, infection, or fracture. Postural stress, disc degeneration, overuse injuries, muscular strains, and lumbar spine biomechanical dysfunctions frequently bring it on. Various factors, including pain perception, socioeconomic conditions, and psychosocial elements such as social isolation, stress, anxiety, depression, and fear-avoidant behaviours, influence the onset and persistence of chronic low back pain (CLBP). Additionally, factors like bad posture, fear of movement, and a sedentary lifestyle are also responsible for developing the symptoms, as these prolong the chronicity and impairment, in addition to increasing the likelihood of developing CLBP.7
Kinesiophobia, or the fear of movement because of the fear of pain or re-injury, is one of the many psychological and physical effects of CLBP that has been shown to have a significant impact on patient recovery and general quality of life.8 Reduced physical activity, greater disability, and poor rehabilitation outcomes are all consequences of kinesiophobia. Its prevalence varies by age, gender, and occupation, which leads to functional limitations and prolonged pain experiences. Adults in their middle years are especially vulnerable to kinesiophobia because of the progression of chronic pain and heightened anxiety about recurrent injuries. The younger adults may also experience it, particularly if they live a sedentary life or have experienced trauma related to injuries in the past.9 A study also reported that women report higher levels of kinesiophobia than men. According to gender differences, most likely as a result of variations in how they perceive pain, react emotionally, and cope.10
The factors like pain severity, functional disability, kinesiophobia, and sleep disturbances 11 in patients with chronic LBP are common and affect the overall health and well-being, and reduce the quality of life of individuals. The rationale for this study stems from comprehending the interplay between these variables. Despite growing awareness of the psychosocial aspects of chronic pain, limited local data are available regarding these associations in CLBP patients.12 Therefore, the objective of this study is to investigate the association between kinesiophobia and pain severity, functional disability, and sleep quality in individuals with chronic low back pain. It is hypothesized that levels of kinesiophobia in patients with chronic lower back pain are positively associated with severity of pain intensity, functional disability, and disturbance of sleep quality. This study is necessary to provide evidence to inform more comprehensive, patient-centred interventions that improve clinical outcomes and enhance the overall quality of life for individuals with CLBP.
Methodology:
The cross-sectional study was conducted over six months from January to June 2025 at the University of Lahore. The data was collected from the medical and physiotherapy outpatient department of the University of Lahore Teaching Hospital, Lahore. This study was conducted following the guidelines of Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) as shown in Figure 1. Ethical approval was obtained from the Research Ethical Committee of the University of Lahore (REC-UOL-/253/08/24). The sample size of 97 was calculated through an online sample size calculator for correlation analysis using the value of the correlation coefficient of kinesiophobia with pain intensity, r=0.281 (13),ꞵ =0.20, and α=0.05 with the given formula; N = [(Zα+Zβ)/C]2 + 3. The participants were recruited through a non-probability convenience sampling technique, and pre-defined eligibility criteria were applied to all the eligible participants to minimise sampling bias. Written informed consent was taken from all the participants at the time of recruitment into the study. The study’s objective was explained to them, and confidentiality and anonymity were ensured, while keeping the right to withdraw from the study.
The inclusion criteria were that the participants were aged 18–60 years, both males and females, having chronic low back pain, persisting for more than 12 weeks,14 with a minimum pain score of 3 or higher on the Numeric Pain Rating Scale (NPRS).15 The exclusion criteria were the presence of a history of fractures or spinal surgery,16 neurological disorders such as Guillain-Barré syndrome, multiple sclerosis, poliomyelitis, etc.15 inflammatory or rheumatic disorders, such as ankylosing spondylitis and rheumatoid arthritis,17 pregnancy or postpartum period, chronic use of powerful analgesics, such as opioids, sleep disorders that are not associated with low back pain, such as sleep apnea or insomnia, history of pain management by physical therapy programs in the last three months or any cognitive disorder or major depressive disorder and other severe mental illnesses that might interfere with the ability to finish the questionnaire.16
The diagnosed patients of chronic LBP were screened using the eligibility criteria, and then the study variables were assessed using a structured questionnaire. Firstly, the demographic details of the study participants were obtained, and then the assessment of pain intensity, functional disability, sleep quality, and kinesiophobia was made through standardised and validated questionnaires.
Kinesiophobia was measured using the Tampa Scale for Kinesiophobia (TSK). It is a valid tool for measuring pain-related fear and disability. It is a 17-item questionnaire with a 4-point Likert scale (1 = strongly disagree, 4 = strongly agree). The total score ranges from 17 to 68, with values ≤37 indicating low kinesiophobia and values >37 representing high kinesiophobia. The higher scores correspond to more avoidance behaviour and a fear of mobility.18
Pain intensity was measured using the Numeric Pain Rating Scale (NPRS), which is a 10-point scale ranging from 0 to 10, with “0” representing no pain to “10” showing the worst pain. The pain severity is classified as mild (1–3), moderate (4–6), and severe (7–10).19
Functional disability was assessed using the Oswestry Disability Index (ODI), a gold-standard tool that evaluates the impact of chronic low back pain on daily functional activities. It has 10 items that cover the various areas of function of daily living, and each item is scored on a 6-point Likert scale from 0–5 points. The total score ranges from 0 to 100, which is expressed in a percentage, with a higher score representing greater disability. Its score is classified as 0–20% as minimal disability, 21–40% as moderate disability, 41–60% as severe disability, 61–80% as crippled, and 81–100% as bedridden.20
Sleep disturbance was assessed using the Pittsburgh Sleep Quality Index (PSQI). The scale comprises 19 items grouped into seven components, each rated on a Likert scale from 0 (no difficulty) to 3 (severe difficulty). Its score ranges from 0 to 21, with a score >5 indicating sleep issues, and higher scores indicating greater sleep disturbances.21
The data analysis was conducted using IBM SPSS version 26. The categorical variables, such as gender, occupation, and presence of LBP, etc., were expressed using frequency or percentage. In contrast, continuous variables, including age, pain intensity, disability, sleep disturbance, and kinesiophobia, were presented as mean and standard deviation along with a histogram.
The normality of data was checked using the graphical methods such as histograms, and Q-Q plots, and statistical tests, i.e., the Kolmogorov-Smirnov test (n≥50). The visual inspection and test results revealed that variable scores were not normally distributed (p < 0.05). Therefore, a non-parametric Spearman correlation was used for analysis and to investigate the relationship between the study variables. The p-value was set as 0.05.
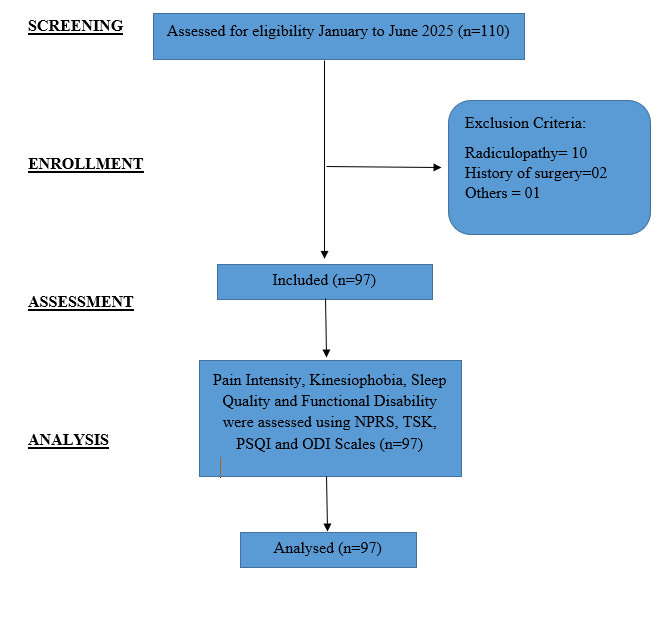
Figure 1: Strobe Flow Diagram
Results:
The mean age of participants was 37.38±7.04 years; there were 47 (48.5%) males and 50 (51.5%) females. The mean BMI of the participants was 22.17 ±1.73 kg/m2. Around 68 (70.1%) were doing jobs, and 44 (45.4%) were working for more than 8 hours. The participants reported a moderate level of pain intensity with a mean of 6.60±1.05, a high level of kinesiophobia with a mean of 41.20±4.39, a moderate level of functional disability with a mean of 35.84±4.85, and a mild sleep disturbance with a mean of 9.52±2.23. The summary of the descriptive statistics for the demographic and outcome variables of the study is shown in Table 1.
A significant relationship was observed between various physical and clinical variables. Height was positively correlated with weight (r = 0.335, p = 0.001) but negatively associated with BMI (r = –0.229, p = 0.024). Height and weight both showed a significant positive correlation with pain intensity (r = 0.352, p = 0.0001; r = 0.206, p = 0.043, respectively). Additionally, kinesiophobia demonstrated significant positive associations with pain intensity, functional disability, and sleep quality. Spearman’s correlation analysis revealed that higher levels of pain (r = 0.294, p = 0.003), greater disability (r = 0.293, p = 0.004), and poorer sleep quality (r = 0.426, p = 0.001) were all significantly related to increased fear of movement. Moreover, sleep quality showed significant positive correlations with pain intensity (r = 0.724, p <0.001) and functional disability (r = 0.552, p <0.001), indicating that individuals experiencing more pain and disability also reported poorer sleep. Additionally, weight (r = 0.242, p = 0.017) and height (r = 0.334, p = 0.001) were moderately associated with disrupted sleep quality. These findings are summarised in Table 2.
| Table 1: Descriptive statistics of Demographic & Outcome Variables | |||
| Study Variables | Frequency(n) | Percentage (%) | |
| Gender | Male | 47 | 48.5 |
| Female | 50 | 51.5 | |
| Occupation of Participants | Business | 10 | 10.3 |
| Job | 68 | 70.1 | |
| Housewife | 11 | 11.3 | |
| Student | 8 | 8.2 | |
| Working hours
per day |
Up to 8 hours | 38 | 39.2 |
| More than 8 hours | 44 | 45.4 | |
| None | 15 | 15.5 | |
| Duration of Pain | Since the Last Three Months | 9 | 9.3 |
| Since the Last Six Months | 63 | 64.9 | |
| More than One Year | 25 | 25.8 | |
| Mean (x̄) | Std. Deviation (SD) | ||
| Age in years | 37.38 | 7.045 | |
| Weight in Kg | 67.49 | 7.113 | |
| Height in cm | 173.32 | 8.952 | |
| Body Mass Index in Kg/m2 | 22.17 | 1.732 | |
| Sleep Quality at PSQI | 9.52 | 2.227 | |
| Pain Intensity at NPRS | 6.60 | 1.046 | |
| Kinesiophobia at TSK | 41.20 | 4.389 | |
| Functional Disability at ODI | 35.84 | 4.854 | |
| Table 2: Correlation Analysis of Demographic and Outcome Variables | |||||||||
| Age | Weight | Height | BMI | NPRS | TSK | ODI | PSQI | ||
| Age | R | – | |||||||
| p-value | |||||||||
| Weight | R | -0.049 | – | ||||||
| p-value | 0.635 | ||||||||
| Height | R | 0.015 | 0.335** | – | |||||
| p-value | 0.887 | 0.001 | |||||||
| BMI | R | -0.126 | 0.112 | -0.229* | – | ||||
| p-value | 0.221 | 0.273 | 0.024 | ||||||
| NPRS | R | -0.133 | 0.206* | 0.352** | -0.109 | – | |||
| p-value | 0.194 | 0.043 | 0.0001 | 0.287 | |||||
| TSK | R | 0.055 | 0.115 | -0.026 | -0.076 | 0.294** | – | ||
| p-value | 0.592 | 0.263 | 0.798 | 0.460 | 0.003 | ||||
| ODI | R | -0.278** | 0.050 | 0.190 | -0.178 | 0.415** | 0.293** | – | |
| p-value | 0.006 | 0.625 | 0.062 | 0.081 | 0.0001 | 0.004 | |||
| PSQI | R | -0.123 | 0.242* | 0.334** | -0.164 | 0.724** | 0.426** | 0.552** | – |
| p-value | 0.231 | 0.017 | 0.001 | 0.109 | <0.001 | <0.001 | <0.001 | ||
Discussion:
This study aimed to determine the relationship of kinesiophobia, pain intensity, functional disability and sleep quality of individuals with chronic low back pain. The results showed that participants had a high level of kinesiophobia, moderate pain intensity and functional disability and mild sleep disturbances. Moreover, a statistically significant correlation of kinesiophobia with the other clinical outcomes of chronic LBP was found, which reflects that the higher levels of kinesiophobia are associated with increased pain intensity, disrupted function, and poor sleep.
Similar findings were seen in the study by John et al., which reported higher levels of kinesiophobia in around 92%, moderate severity of back pain, and a moderate level of functional disability.9 In the same way, Varallo et al. stated that kinesiophobia plays a mediating role between pain and function in chronic low back pain. Their findings suggest that fear of movement not only coexists with pain and disability but also serves as a psychological mechanism through which pain contributes to greater functional limitation.13 Additionally, Alshahrani and Reddy demonstrated that individuals with CLBP experienced high levels of kinesiophobia, which was significantly associated with impaired functional balance and reduced postural stability. However, their study population consisted primarily of older adults with underlying osteoporosis, which may have influenced the severity of outcomes.22
In parallel to the results of the current study, Luque-Suarez et al. observed that the positive correlation of kinesiophobia with pain severity and functional disability in chronic shoulder pain patients.23 Although both studies have covered different anatomical regions, both highlight the persistent influence of kinesiophobia on pain perception and functional ability across various musculoskeletal conditions. Likewise, Mekonnen et al. identified the predictive factors of kinesiophobia and reported that high BMI, severe pain intensity, and physical inactivity significantly contributed to its development.14 The current study also observed that the participants with high BMI and moderate levels of pain and functional disability tended to report higher levels of kinesiophobia.
Consistent with the findings of the present study, a study by Pazzinatto et al. demonstrated a significant association between kinesiophobia and clinical outcomes in individuals with patellofemoral pain syndrome, highlighting that higher levels of kinesiophobia were linked to increased BMI, pain catastrophizing, lower levels of physical activity, and reduced quality of life.8 Similarly, a study by Wlazło et al. highlighted that movement-related fear is prevalent among individuals suffering from chronic non-communicable diseases. However, their study population differed from the current research, focusing on non-musculoskeletal, systemic chronic conditions. In contrast, the present study investigated individuals with a musculoskeletal condition, i.e., chronic low back pain.24
Limitations: Although the study was conducted with care, following the ethical considerations and clinical guidelines, there are still a few limitations of this study. The study had a small sample size owing to time restrictions of the study and resources. This study was conducted, and data were collected from a single city using the convenience sampling technique, which might interfere with the generalizability of findings. Furthermore, the outcome variables tools were of a subjective nature that may influence the response, as every individual has their threshold to a stimulus.
Recommendation: Based on the findings of study, it is recommended to clinicians to regularly assess the level of kinesiophobia, and educate the patients with chronic low back pain or other musculoskeletal disorders about the benefits of movement, and side effects of stasis, so that the fear of movement can be controlled to reduce the impact of pain, and restoration of the function and overall well-being. It is advised to the community to add mild physical activity in their daily routine, despite chronic pain, as the absence of activity is likely to increase the clinical outcomes of chronic LBP.
Conclusion:
It is concluded that there is a correlation of kinesiophobia with pain intensity, functional disability, and sleep quality. The greater severity of kinesiophobia is related to a higher level of pain intensity, more disturbances in physical function, and poorer sleep quality.
References:
- Chen S, Chen M, Wu X, Lin S, Tao C, Cao H, et al. Global, regional and national burden of low back pain 1990–2019: a systematic analysis of the Global Burden of Disease study 2019. J Orthop Translat. 2022; 32:49–58.
- Pang H, Chen S, Klyne DM, Harrich D, Ding W, Yang S, et al. Low back pain and osteoarthritis pain: a perspective of estrogen. Bone Res. 2023;11(1):42.
- Kahere M, Hlongwa M, Ginindza TG. A scoping review on the epidemiology of chronic low back pain among adults in sub-Saharan Africa. Int J Environ Res Public Health. 2022;19(5):2964.
- Saravanan A, Bajaj P, Matthews HL, Tell D, Starkweather A, Janusek L. Fatigue and depressive mood in chronic low back pain. Pain Manag Nurs. 2024;25(3):225–30.
- Ammer K, Ebenbichler G, Bochdansky T. Low back pain—a disease or condition of impaired functional health? Definition-inherent consequences for the comprehensive care of back pain patients. Biomed. 2022;2(2):270–81.
- Frizziero A, Pellizzon G, Vittadini F, Bigliardi D, Costantino C. Efficacy of core stability in non-specific chronic low back pain. J Funct Morphol Kinesiol. 2021;6(2):37.
- Baradaran Mahdavi S, Riahi R, Vahdatpour B, Kelishadi R. Association between sedentary behavior and low back pain: a systematic review and meta-analysis. Health Promot Perspect. 2021;11(4):393–410.
- Pazzinatto MF, Silva DD, Willy RW, Azevedo FM, Barton CJ. Fear of movement and (re)injury is associated with condition-specific outcomes and health-related quality of life in women with patellofemoral pain. Physiother Theory Pract. 2022;38(9):1254–63.
- John JN, Ugwu EC, Okezue OC, Ekechukwu EN, Mgbeojedo UG, John DO, et al. Kinesiophobia and associated factors among patients with chronic non-specific low back pain. Disabil Rehabil. 2023;45(16):2651–9.
- Botta AFB, Da Silva JC, Lopes HS, Boling MC, Briani RV, De Azevedo FM. Group- and sex-related differences in psychological and pain processing factors in people with and without patellofemoral pain: correlation with clinical outcomes. BMC Musculoskelet Disord. 2023;24(1):397.
- Ilyas N, Jamil A, Akram S, Ilyas R, Afzal Z, Akram A. Comparative effects of hold relax with agonist contraction and active release therapy on pain, functional disability, and sleep quality in piriformis syndrome: hold relax versus active release in piriformis syndrome. South J Phys Ther Rehabil. 2024; 4:22–6.
- Wettstein M, Eich W, Bieber C, Tesarz J. Pain intensity, disability, and quality of life in patients with chronic low back pain: does age matter? Pain Med. 2019;20(3):464–75.
- Varallo G, Scarpina F, Giusti EM, Cattivelli R, Guerrini Usubini A, Capodaglio P, et al. Does kinesiophobia mediate the relationship between pain intensity and disability in individuals with chronic low-back pain and obesity? Brain Sci. 2021;11(6):684.
- Mekonnen Y, Gashaw M, Abich Y, Takele MD, Chanie ST, Wayessa DI, et al. Kinesiophobia and associated factors among people with musculoskeletal disorders in Ethiopia: a multicenter cross-sectional study. BMC Musculoskelet Disord. 2025;26(1):55.
- Sakulsriprasert P, Vachalathiti R, Kingcha P. Association among pain, disability, and functional capacity in patients with chronic non-specific low back pain: a cross-sectional study. Biomed Res. 2021;34(1):149–57.
- Shenoy NN, Kumar KD, Kovela RK. The relationship between kinesiophobia, pain intensity and functional disability among elderly individuals with low back pain: a cross-sectional study. J Clin Diagn Res. 2024 ;18(1): YC01–YC03.
- Liechti M, Menegon M, Schurz AP, Taeymans J, Baur H, Clijsen R, et al. Association between pain intensity and body composition in adults with chronic non-specific low back pain: a systematic review and meta-analysis. Obes Rev. 2025;26(4): e13875.
- Eiger B, Errebo M, Straszek CL, Vaegter HB. Less is more: reliability and measurement error for three versions of the Tampa Scale of Kinesiophobia (TSK-11, TSK-13, and TSK-17) in patients with high-impact chronic pain. Scand J Pain. 2023;23(1):217–24.
- Atisook R, Euasobhon P, Saengsanon A, Jensen MP. Validity and utility of four pain intensity measures for use in international research. J Pain Res. 2021; 14:1129–39.
- Koivunen K, Widbom-Kolhanen S, Pernaa K, Arokoski J, Saltychev M. Reliability and validity of Oswestry Disability Index among patients undergoing lumbar spinal surgery. BMC Surg. 2024;24(1):13.
- Akobundu UN, Oledibe OJ, Obiekwe SJ, Okonkwo UP, Amaechi IA, Daniel JA, et al. Cross-cultural adaptation and validation of the Pittsburgh Sleep Quality Index (PSQI) in the Igbo language. Discov Psychol. 2024;4(1):154.
- Alshahrani MS, Reddy RS. Kinesiophobia, limits of stability, and functional balance assessment in geriatric patients with chronic low back pain and osteoporosis: a comprehensive study. Front Neurol. 2024; 15:1354444.
- Luque-Suarez A, Martinez-Calderon J, Navarro-Ledesma S, Morales-Asencio JM, Meeus M, Struyf F. Kinesiophobia is associated with pain intensity and disability in chronic shoulder pain: a cross-sectional study. J Manipulative Physiol Ther. 2020;43(8):791–8.
- Wlazło M, Szlacheta P, Grajek M, Staśkiewicz-Bartecka W, Rozmiarek M, Malchrowicz-Mośko E, et al. The impact of kinesiophobia on physical activity and quality of life in patients with chronic diseases: a systematic literature review. Appl Sci. 2025;15(4):2086.
Copyright PolicyAll Articles are made available under a Creative Commons “Attribution-NonCommercial 4.0 International” license. (https://creativecommons.org/licenses/by-nc/4.0/). Copyrights on any open access article published by Journal Riphah college of Rehabilitation Science (JRCRS) are retained by the author(s). Authors retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means; provided the article is correctly cited. JRCRS does not allow commercial use of the articles published. All articles published represent the view of the authors and do not reflect the official policy of JRCRS.