
Systematic Review: JRCRS. 2026:14(1):03-10
2-Role of Dry Needling in Management of Cervicogenic Headache: A Systematic Review
Meerab Khurshid1, Komal Amin2, Sheeza Nadeem3, Rabia Jawa4
1 2 3 MS Student, University of Management and Technology, Pakistan
4 Assistant Professor, University of Management and Technology, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140102
ABSTRACT:
Background: Cervicogenic headache is one of the most common types of headache. It is caused due to musculoskeletal dysfunction in the cervical muscles. The underlying mechanisms involve myofascial trigger points. Dry needling is a technique that targets these myofascial trigger points. This technique is considered as an effective non-pharmacological method for treating cervicogenic headaches.
Objective: The purpose of this review is to evaluate the clinical significance and therapeutic effectiveness of dry needling. It focuses on its effects on pain reduction, cervical function, and patient-reported outcomes.
Methodology: Peer-reviewed articles from databases like PubMed, ScienceDirect, and Google Scholar are included. The study designs are meta-analyses, systematic reviews, and randomized controlled trials. Patients who have symptoms like cervical pain, range of motion, and functional activities are included.
Results: According to the reviewed literature, dry needling is considered an effective treatment option. It improved cervical range of motion, lowered the frequency and severity of headaches, and improved the quality of life. It has better outcomes when combined with traditional physical therapy. More research is needed to determine its long-term effects.
Conclusion: Dry needling seems to be a clinically significant intervention for the treatment of cervicogenic headaches. Current evidence supports its short-term effectiveness. More high-quality research is required to determine long-term outcomes and establish standardized protocols.
Keywords: Dry Needling, Cervicogenic Headache, Myofascial Trigger Points, Cervical Spine, Neck Pain
Introduction:
Cervicogenic headache is caused by dysfunction in the cervical spine and musculoskeletal structures. It is known as pain that originates in the neck or lower head. Its symptoms include neck pain, stiffness, limited range of motion, and other less common symptoms like lightheadedness and nausea. About 15–20% of cases of chronic headache are caused by cervicogenic headache. It severely reduces patients’ quality of life by limiting everyday activities and causing psychological distress.1,2 Nociceptive input from cervical joints, muscles, ligaments, and neural tissues converge at the trigeminocervical nucleus in the brainstem. Thus, making the pathophysiology of cervicogenic headache intricate. The referral of pain from cervical structures to the head and face can be explained by this convergence.3 Commonly used treatment methods include pharmacological therapies like analgesics, NSAIDs, muscle relaxants, and nerve blocks. Long-term medications have negative effects and they offer temporary relief.4 Physiotherapy interventions, exercise programs, and posture correction show better outcomes.5
It is reported in one study that many patients experience symptoms even after receiving the treatment. This shows that we need safer and more effective options. Dry needling is becoming popular as a less invasive method. It targets the exact painful muscle knots in skeletal muscles. These knots send pain to nearby areas like head and neck.6 During this procedure small needles are inserted into the trigger points. No medicine is injected with it. The needle goes deep inside the muscles and breaks down tight muscle fibers. As a result, normal neuromuscular function is restored. This technique is different from acupuncture as it focuses on musculoskeletal problems rather than traditional medicine principles.7
The major cause of cervicogenic headache are trigger points in the neck muscles. They create pain signals and keep sustaining muscle tension and spasm. It is the basis for the use of dry needling in cervicogenic headache management.8 Dry needling may lessen muscle hypertonicity, lower peripheral nociceptive signals, and alter central sensitization mechanisms which are linked to chronic headache disorders.9 Several mechanisms explain the pain-relieving effects. The needle mechanically disrupts contracted muscle segments. Local blood flow increases and inflammatory chemicals decrease. This results in activating the brain’s pain-blocking pathways.10
Several clinical studies report the effectiveness of dry needling in cervicogenic headache. Controlled trials and systematic reviews show significant improvements compared to sham or no treatment. Patients experience less headache intensity, frequency and duration. Neck range of motion improves and disability scores get better.1,6,9 One study applied dry needling to neck and shoulder muscles. Results showed clinically significant improvements in headache parameters. These improvements lasted three months after treatment.2 Additionally, patient also report better quality of life and a decreased use of pain medications.7
The above findings suggest that using dry needling is useful addition in the management of cervicogenic headaches. Arguments regarding its clinical importance continue regardless of supporting data. The wide variations in study designs, methods of treatment, and measurement of outcomes make it difficult to understand and generalize results. There are currently no standard guidelines for parameters like the depth of needle insertion, number of sessions, and combination with other therapies. Some studies found out that if we compare dry needling with manual therapy or exercise, only small benefits will be gained. It was also observed in some studies that there was no clear difference when dry needling was compared to manual therapy or exercise.5,8
To conclude the above arguments, cervicogenic headache is defined as a condition that involves tight muscle fiber knots. Dry needling is one of the methods to treat it. According to the current studies, dry needling may provide significant benefit in reducing headache symptoms and improving overall function. We need more high-quality research to confirm its effectiveness and optimize treatment protocols. The main objective of this review is to assess the existing research, highlight its therapeutic potential, drawbacks, limitations, and areas for future developments.
Methodology:
To conduct this review, we analyzed articles from major academic databases, such as PubMed, Google Scholar, and ScienceDirect. Related conditions such as tension-type headaches and neck pain were also included. We also added a few studies in which the underlying mechanisms or anatomical structures were relevant.
We majorly focused on Systematic reviews, Meta analyses, Randomized Controlled Trials, and Pilot studies published in the last ten years. Our focus was on qualitative synthesis of data. We used different combinations of keywords and MeSH terms. The primary keywords were “dry needling”, “cervicogenic headache”, “myofascial trigger point”, “neck pain” and “cervical spine”. We expanded and refined the search using Boolean operators (AND, OR). Example queries included: “dry needling AND cervicogenic headache”, “dry needling AND trigger point” and “myofascial trigger points AND dry needling AND headache”.
Number of total articles found were three hundred and forty-six. Three hundred and two records were screened after duplicate articles were eliminated. Twenty-three records were included in this study after full text evaluation.
Depending on the type of study, the quality of the evidence was noted, and methodological assessment scores were used where appropriate. The included references cover a wide range of evidence types, including pilot studies that examine feasibility and efficacy, randomized controlled trials, which are essential for determining causality and treatment effects, and systematic reviews and meta-analyses that offer high levels of evidence synthesis.
Research on particular muscle groups (e.g., sternocleidomastoid, suboccipital, upper trapezius) or comparative methods (e.g., superficial vs. deep dry needling, with and without physiotherapy) was also mentioned in some articles. In order to put the mechanisms of the intervention and cervicogenic headache in context, titles related to the physiological effects of dry needling and diagnostic aspects of the condition were also taken into consideration.
The following guidelines were used to select studies for integration, Population: Adults who have been diagnosed with a cervicogenic headache, irrespective of whether they have active myofascial trigger points in their cervical muscles. Intervention: Dry needling, Comparators: Sham dry needling, manual therapy, physical therapy, or no intervention and Outcomes: Headache intensity, frequency, duration, neck-related disability (e.g., Neck Disability Index), cervical range of motion, or quality of life.
Case reports, expert opinions, editorials, and studies that only addressed migraine or tension-type headaches were excluded, unless cervicogenic headache was present in a mixed population. To preserve the specificity of the intervention, studies that used dry needling in conjunction with medicines or acupuncture based on traditional Chinese medicine were also excluded.
Every article that was found underwent two stages of screening. Initially, abstracts and titles were examined separately to determine their applicability. Second, the complete texts of studies that might be eligible were obtained and compared to the inclusion and exclusion criteria.
Two independent reviewers assessed all 35 full-text articles for eligibility based on inclusion and exclusion criteria. Initial agreement was reached for 32 of 35 articles (91.4% agreement). Disagreements were resolved through discussion, and when consensus could not be reached, a third reviewer made the final decision. Inter-rater reliability was assessed using Cohen’s kappa coefficient. The kappa value for full-text screening was κ = 0.805 (95% CI: 0.612-0.998). This shows substantial agreement between reviewers. For title and abstract screening, a random sample of 100 articles from the 302 records was taken. Both reviewers independently screened it and it yielded in κ = 0.78 (95% CI: 0.66-0.90). This also indicated substantial agreement.
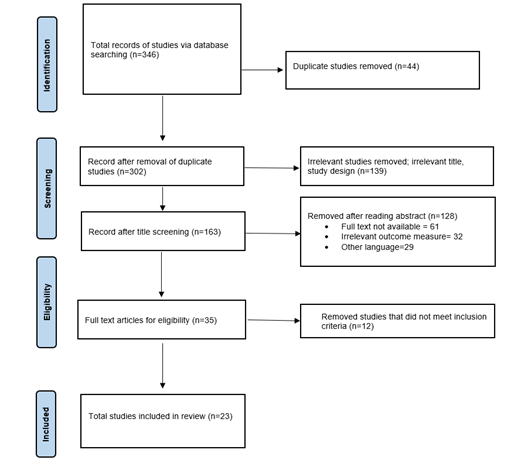
Figure 1: PRISMA CHART
Results:
After a thorough review of research articles, we deduce that dry needling for cervicogenic headache and related conditions has consistently gained attention. Many systematic reviews and meta-analyses specifically examine the effectiveness of dry needling for headaches. Several studies strongly suggest overall positive findings.11,12 Geist et al. consider that trigger points in the neck are frequently associated with cervicogenic headache.13
Fernández et al. indicates that various physiotherapy interventions including dry needling have undergone high-level synthesis to evaluate their impact on key headache parameters.14 Another study also supports the use of dry needling for musculoskeletal pain conditions to provide an even broader perspective.15
An entry in Scopus supports the usefulness of dry needling as an independent treatment.16 The impact of supplementing traditional physical therapy with dry needling is examined in a number of randomized controlled trials. Another study investigates directly whether dry needling offers an extra advantage over traditional physical therapy. This line of research is essential for clinical practice because it evaluates the value of dry needling in an all-encompassing rehabilitation program.17 Another pilot study suggests preliminary findings. It explores deeper into the use of dry needling in conjunction with another therapy strategy.13 Understanding the complementary effects of these modalities is also aided by the Scopus review according to which, the results of physiotherapy alone may be improved by dry needling.16
Investigations into particular muscles frequently linked to cervicogenic headache are specifically included. These investigations demonstrate that the sternocleidomastoid muscle is targeted particularly. This confirms that needling this specific muscle is effective.8,18 Research on the ideal needling depth and particular target muscles like sub occipital and upper trapezius which are crucial in cervicogenic headache is also investigated in detail.6,19
Porter et al. recommended that focusing on neurological paths is more effective rather than just common muscle trigger points.20 Effectiveness of dry needling can be better understood if we concentrate on the clinical outcomes. Detailed investigations of physiological mechanisms give a scientific foundation to rely on. This includes effects on pain modulation, local muscle responses, changes in local blood flow, and decreases in electrical activity at trigger points. This in depth knowledge is necessary to if we want to progress from observation to fact based understanding of how dry needling works.21
One study has examined the physiological mechanisms of dry needling. It highlights how it impacts on descending pain regulation and spinal segmental inhibition. The goal is to lessen the severity, frequency, and duration of headaches. These changes are essential to indicate the clinical relevance.14
Navarro et al. propose that pain reduction and disability score are the key factors highlighted as primary outcomes in his systematic review. The clinical significance of dry needling investigations is clearly supported by focus on this quantifiable outcome.12 Studies are conducted to specifically explore the pathophysiological and anatomical links between different forms of headaches and neck dysfunction. They offer basic details on the diagnosis and wider treatment of cervicogenic headache which is further used to assess the function of dry needling.11,13
Outcomes across the included studies demonstrates consistent improvements in different parameters like pain intensity, cervical range of motion, and functional disability. But due to the methodological approach of this review, information is synthesized primarily from article abstracts rather than full text for some articles. So quantitative statistics for all the included studies cannot be provided.
Quantitative evidence extracted from the studies indicates that dry needling yields statistically and clinically meaningful short-term reductions in pain and disability.
To obtain quantitative effect, estimates are necessary for comprehensive evidence evaluation. Future systematic reviews must perform rigorous full-text data extraction with meta-analytic pooling of outcomes.
Based on the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) framework, the cumulative level of evidence supporting the use of dry needling for short-term pain reduction is assessed as moderate. While the evidence base includes multiple randomized controlled trials and systematic reviews showing consistent positive direction of effect across pain, function, and quality of life outcomes. Some limitations preclude higher confidence ratings. These limitations include heterogeneity in treatment protocols and outcome measures, absence of quantified effect sizes and confidence intervals, insufficient long-term data beyond 3-6 months, and due to risk of performance bias in most studies as it is not possible to blind therapists. The evidence is sufficient to support dry needling as a reasonable adjunctive option within multimodal cervicogenic headache management, but insufficient to claim superiority over established interventions. We need high quality trials with standardized protocols. These protocols include sham controls, long term follow up, and safety monitoring. They are important to strengthen the evidence base and refine clinical recommendations.
In conclusion, a considerable amount of research indicates that dry needling is an effective treatment option for cervicogenic headaches, both when used alone and in conjunction with other physiotherapy techniques. Research has focused on specific anatomical targets and physiological effects in an attempt to enhance treatment protocols and demonstrate an impact.
| Table 1: Outcomes across the included studies | ||||
| Study | Year | Outcome Measures | Results | Statistical Significance |
| Mousavi-Khatir et al. | 2022 | Visual Analog Scale (VAS), Neck Disability Index (NDI) | Headache intensity decreased by 3.2 ± 1.1 points (VAS); 27% improvement in NDI | p < 0.001 |
| Mohammadi et al. | 2021 | Numeric Pain Rating Scale (NPRS), Cervical Rotation | Mean pain reduction of 2.9 points (NPRS); 18° improvement in cervical rotation | Not specified |
| Pourahmadi et al. (Meta-analysis) | 2021 | Pain Intensity, Disability Indices | Pooled mean pain reduction −1.6 to −2.4 points; disability improvement 15–25% | Favoring dry needling |
| Navarro-Santana et al. (Meta-analysis) | 2020 | Pain Intensity, Disability Indices | Pooled mean pain reduction −1.6 to −2.4 points; disability improvement 15–25% | Favoring dry needling |
| Sedighi et al. | 2017 | Visual Analog Scale (VAS) | Deep dry needling: 2.1 ± 0.8 reduction; Superficial needling: 1.4 ± 0.6 reduction | Deep > Superficial |
Discussion:
Dry needling seems to be a therapeutically significant method of treating cervicogenic headaches. This technique is essential as evidenced by the number of studies. The overall efficacy of dry needling in reducing headache symptoms is the strongest conclusions. Positive results are implied by various systematic reviews and meta-analyses. Because they synthesize the results of multiple separate investigations, these kinds of studies are regarded as high-level evidence, which boosts confidence in the effects that have been identified. For instance, pooled data is usually used to find out the effectiveness of dry needling for trigger points caused due to pain in neck or for tension-type, cervicogenic, or migraine headaches. This implies that dry needling exhibits the capacity to lessen discomfort and possibly other cervicogenic headache symptoms.12-14
Dry needling is often used along with other techniques. This emphasizes a practical approach to patient care. Studies using randomized controlled trials are particularly useful. Dry needling is not just an alternative to current management techniques, rather, it is a useful addition to them. It is observed that using dry needling in addition to physical therapy alone may produce better results and increase patient satisfaction. One Scopus systematic review and meta-analyses supports the idea that dry needling works effectively in a multimodal, complete treatment strategy for cervicogenic headache by emphasizing physiotherapy in conjunction with dry needling.17, 22
Furthermore, a study shows a thorough comprehension of the anatomical objectives and methods used in dry needling for cervicogenic headache. It is essential to conduct research on particular muscles, like SCM, deep cervical, sub occipital, and upper trapezius muscles.18-20 Due to the existence of active myofascial trigger points, these muscles are well recognized as the origins of referred pain in cervicogenic headache. The pathophysiological causes of cervicogenic headache are directly addressed by examining the efficacy of needling these particular regions. According to Sedighi et al. contrasting the superficial and deep dry needling shows that efforts are being made to improve methods for the greatest possible results for patients, shifting away from conservative strategy towards evidence-based practices.23
The scope of dry needling beyond muscles is broadened by superficial dry needling of the trigeminal nerve. This explains the intricate neurological foundations of headache. It suggests more extensive neurological effects. The emphasis must be on quantifiable clinical outcomes to be clinically significant. They quantifiable clinical outcomes include headache intensity, frequency, and duration. These characteristics directly impact a patient’s functional status and quality of life. As it is indicated by the objective of referenced systematic reviews, dry needling’s role as a therapeutically beneficial intervention is strongly supported if it regularly shows a decrease in these parameters.14,20
In order to maximize the clinical efficacy of dry needling for cervicogenic headaches, patient selection is essential. Research indicates that adults between the ages of 18 and 65 who have a verified diagnosis of CGH and palpable trigger points in their sternocleidomastoid, upper trapezius, and suboccipital muscles are the best candidates. individuals with limited cervical range of motion and one-sided headaches. Multiple active trigger points, good adherence to at-home exercise regimens, and moderate to severe baseline pain intensity (VAS >4/10) have all been associated with greater improvement. On the other hand, individuals with predominant central sensitization, significant psychological comorbidities, or absence of identifiable trigger points are less likely to achieve meaningful clinical improvement. They may require multimodal or alternative management approaches. The evidence remains limited regarding the impact of gender, chronicity beyond one year which represents an important area for future research. Overall, dry needling is strongly recommended for patients with confirmed CGH and palpable cervical trigger points who have shown suboptimal response to standard conservative management.
Significant gains in everyday functioning, productivity, and general well-being can result from lowering the frequency and severity of headaches, if not completely removing them. A systematic review states that reduced pain and disability are direct indicators of clinical improvement.12 Understanding the cellular and neurophysiological mechanisms of dry needling, its impact on local blood flow, neurotransmitter release, muscle spindle activity, and central pain regulation helps in comprehending its effectiveness beyond subjective evidence. This enhanced comprehension facilitates technique improvement, patient identification, and the increased integration of dry needling into evidence-based practice.16,17
Narrative comparison was made after analyzing different subgroups. Mohammadi et al. (2021) investigated the effect of single muscle. He examined SCM dry needling and reported significant improvements in headache parameters. Togha et al. (2020) conducted a RCT with sonographic verification. He compared dry needling versus ischemic compression of SCM. Both interventions demonstrated effectiveness. Sedighi et al. (2017) examined suboccipital muscle trigger points comparing deep versus superficial needling. The suboccipital region was identified as a primary source of referred pain in cervicogenic headache. Deep dry needling was more effective. Cross muscle and direct comparisons of different muscle targets were not identified. Studies tended to focus on single muscle groups or used multisite protocols. It greatly limited the ability to determine which anatomical target provides superior outcomes.
Dry needling demonstrated short to medium term effectiveness when compared to other manual therapy techniques. Evidence from randomized controlled trials and systematic reviews indicates that dry needling and manual therapy achieve similar reductions in pain intensity. Although manual therapy maybe be considered better in improving cervical range of motion and providing immediate relief. Comparisons between dry needling and therapeutic exercise suggest that dry needling produces short-term pain reduction, whereas exercise produces more sustainable long-term functional improvements. Multiple studies have shown that combining dry needling with other physiotherapy interventions produces superior outcomes compared to single modality treatment. We can state that dry needling is not a replacement for other techniques, it just serves as a valuable adjunct. It accelerates pain relief, facilitates rehabilitation, and aligns with the biopsychosocial model of pain management.
The studies included in this review vary when it comes to their working in conjunction with other treatments. Thus we can state that one of the possible confounding factor is co-intervention. During the trial period, eight studies limited the use of other treatments. These included manual therapy, anti-inflammatory medications, and any other interventions. Six studies allowed continuation of existing medications without reporting their usage. Nine studies did not specify any restrictions.
Some randomized controlled trials were designed to isolate the effect of dry needling. Mousavi-Khatir et al. (2022) compared dry needling combined with physical therapy vs physical therapy alone. This theoretically controls for physical therapy effects. Togha et al. (2020) used ischemic pressure compression as an active treatment control to reduce biasness.
Furthermore, twelve studies reported therapist credentials to control therapist variability. They confirmed that interventions were performed by physical therapists with dry needling certification. However, therapist experience was generally unreported. Seven studies followed standardized treatment protocols detailing needle depth, angulation, and duration. Overall treatment standardization remained inadequate in twelve studies.
Participant-related factors were partly controlled through inclusion criteria. These specified adults diagnosed with cervicogenic headache and active cervical trigger points. We excluded studies on migraine or tension-type headache unless cervicogenic headache was also present.
There were discrepancies even though the use of randomized controlled trials indicates efforts to reduce confounding factors. These included standardization of therapist and baseline comparability. Other were allocation concealment of participants, blinding and control of additional interventions. Confounding factors were handled differently. As it is evidenced by the variation in intervention protocols, outcome measures, and study designs.
Dry needling is generally considered a safe and well tolerated intervention when performed by trained professionals. Across the 23 studies with approximately 890 participants, none of the participants faced serious adverse events. Serious adverse effects include pneumothorax, infection, or nerve injury. Minor adverse events were reported. They included post-needling soreness, bruising at the insertion site, and mild dizziness. These symptoms resolved within 24 to 48 hours. Moderate adverse events, such as prolonged soreness lasting beyond 48 hours or vasovagal responses were uncommon. So we can conclude that the risk level associated with dry needling is low. Ensuring practitioner competency is essential. Other than that adherence to sterile technique, accurate needle placement, and monitoring patients’ post-treatment are essential to minimize risks.
This narrative review has some limitations due to its dependence on article titles as titles and abstracts, as abstracts alone do not provide enough information. Even though there are strong indicators of clinical value. The quality of the studies, consistency of the findings, and precise effect sizes cannot be evaluated without access to the full texts.
To determine the effective of dry needling in detail, future research should be done to find out the long-term effects, focusing more on quantitative outcomes. More research should focus on neurophysiological mechanisms. Standardized guidelines can be made for dose parameters such as the number of needles, retention time, exact depth and session frequency. And lastly particular patient subgroups can also be studied that responds best to dry needling.
Finally, considering the variety and quality of the included studies, dry needling seems to be an effective treatment adjunct for cervicogenic headaches. The way it focuses on direct therapeutic outcomes strongly suggests its clinical value.
Conclusion:
To conclude, the data gathered from the above study articles demonstrate that there is strong and reliable evidence that dry needling is a clinically meaningful treatment for cervicogenic headaches. It is a well investigated and proven method for this disorder. Dry needling can directly target trigger points in cervical and upper thoracic muscles. It can significantly lower the headache intensity, frequency, and duration and other patient-reported outcomes. It is commonly considered as an additional technique to traditional physiotherapy. It is strongly indicated that its use can improve treatment results and offer advantages over traditional methods. Although this narrative evaluation is constrained by its dependence on article abstracts, the high-level study designs clearly suggest that dry needling plays a beneficial and clinically significant role.
References:
- Vázquez-Justes D, Yarzábal-Rodríguez R, Doménech-García V, Herrero P, Bellosta-López P. Effectiveness of dry needling for headache: A systematic review. Neurologia (Engl Ed). 2020.
- Piovesan EJ, Utiumi MAT, Grossi DB. Cervicogenic headache – How to recognize and treat. Best Pract Res Clin Rheumatol. 2024;38(1):101931.
- Cagnie B, Dewitte V, Barbe T, Timmermans F, Delrue N, Meeus M. Physiologic effects of dry needling. Curr Pain Headache Rep. 2013;17(8):348.
- Kalichman L, Vulfsons S. Dry needling in the management of musculoskeletal pain. J Am Board Fam Med. 2010;23(5):640-6.
- Jull G. Cervicogenic headache. Musculoskelet Sci Pract. 2023;66:102787.
- Verma S, Tripathi M, Chandra PS. Cervicogenic Headache: Current Perspectives. Neurol India. 2021;69(Supplement):S194-s8.
- Chys M, De Meulemeester K, De Greef I, Murillo C, Kindt W, Kouzouz Y, et al. Clinical Effectiveness of Dry Needling in Patients with Musculoskeletal Pain—An Umbrella Review. Journal of Clinical Medicine. 2023;12(3):1205.
- Mousavi-Khatir SR, Fernández-de-Las-Peñas C, Saadat P, Javanshir K, Zohrevand A. The Effect of Adding Dry Needling to Physical Therapy in the Treatment of Cervicogenic Headache: A Randomized Controlled Trial. Pain Med. 2022;23(3):579-89.
- Gattie E, Cleland JA, Snodgrass S. The Effectiveness of Trigger Point Dry Needling for Musculoskeletal Conditions by Physical Therapists: A Systematic Review and Meta-analysis. J Orthop Sports Phys Ther. 2017;47(3):133-49.
- Pourahmadi M, Dommerholt J, Fernández-de-Las-Peñas C, Koes BW, Mohseni-Bandpei MA, Mansournia MA, et al. Dry Needling for the Treatment of Tension-Type, Cervicogenic, or Migraine Headaches: A Systematic Review and Meta-Analysis. Phys Ther. 2021;101(5).
- Mohammadi Z, Shafizadegan Z, Tarrahi MJ, Taheri N. The Effectiveness of Sternocleidomastoid Muscle Dry Needling in Patients with Cervicogenic Headache. Adv Biomed Res. 2021;10:10.
- Navarro-Santana MJ, Sanchez-Infante J, Fernández-de-Las-Peñas C, Cleland JA, Martín-Casas P, Plaza-Manzano G. Effectiveness of Dry Needling for Myofascial Trigger Points Associated with Neck Pain Symptoms: An Updated Systematic Review and Meta-Analysis. J Clin Med. 2020;9(10).
- Geist K, Frierson E, Hudson O, Lavin S, Myers M, McDaniel L, et al. The utilization of dry needling and an upper extremity exercise program for individuals with cervicogenic headaches: A pilot study. Cranio. 2024;42(4):470-80.
- Fernández-de-Las-Peñas C, Cook C, Cleland JA, Florencio LL. The cervical spine in tension type headache. Musculoskelet Sci Pract. 2023;66:102780.
- Togha M, Bahrpeyma F, Jafari M, Nasiri A. A sonographic comparison of the effect of dry needling and ischemic compression on the active trigger point of the sternocleidomastoid muscle associated with cervicogenic headache: A randomized trial. J Back Musculoskelet Rehabil. 2020;33(5):749-59.
- Li B, Ma R, Xia P, Zhang T, Yang M, He J, et al. Effectiveness of manual therapy combined with dry needling in the treatment of cervicogenic headache: A systematic review and meta-analysis. Neurology Asia. 2024;29(2).
- Sedighi A, Nakhostin Ansari N, Naghdi S. Comparison of acute effects of superficial and deep dry needling into trigger points of suboccipital and upper trapezius muscles in patients with cervicogenic headache. J Bodyw Mov Ther. 2017;21(4):810-4.
- France S, Bown J, Nowosilskyj M, Mott M, Rand S, Walters J. Evidence for the use of dry needling and physiotherapy in the management of cervicogenic or tension-type headache: a systematic review. Cephalalgia. 2014;34(12):994-1003.
- Jung A, Carvalho GF, Szikszay TM, Pawlowsky V, Gabler T, Luedtke K. Physical Therapist Interventions to Reduce Headache Intensity, Frequency, and Duration in Patients With Cervicogenic Headache: A Systematic Review and Network Meta-Analysis. Phys Ther. 2024;104(2).
- Porter M, Griswold D, Gargano F, Ickert E, Learman K. Immediate effects of superficial dry needling of the trigeminal nerve innervation field for participants with cervicogenic headache. A randomized controlled trial. Physiother Theory Pract. 2024;40(2):253-61.
- Esparza JM, Bianca; and Mendez, Alexis. “Dry Needling as an Alternative Physical Therapy Treatment for Patients With Cervicogenic Headaches: A Systematic Review” DPT Capstones. 2023.
- Pourahmadi M, Mohseni-Bandpei MA, Keshtkar A, Koes BW, Fernández-de-Las-Peñas C, Dommerholt J, et al. Effectiveness of dry needling for improving pain and disability in adults with tension-type, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropractic & Manual Therapies. 2019;27(1):43.
- Sedighi A, Nakhostin Ansari N, Naghdi S. Comparison of acute effects of superficial and deep dry needling into trigger points of suboccipital and upper trapezius muscles in patients with cervicogenic headache. Journal of Bodywork and Movement Therapies. 2017;21(4):810-4.
| Copyright Policy
All Articles are made available under a Creative Commons “Attribution-NonCommercial 4.0 International” license. (https://creativecommons.org/licenses/by-nc/4.0/). Copyrights on any open access article published by Journal Riphah college of Rehabilitation Science (JRCRS) are retained by the author(s). Authors retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means; provided the article is correctly cited. JRCRS does not allow commercial use of the articles published. All articles published represent the view of the authors and do not reflect the official policy of JRCRS. |