
Original Article: JRCRS. 2025; 13(4):246-251
10- Clinical Approaches and Return to Sport Guidelines Following Anterior Cruciate Ligament Reconstruction: A Survey of Pakistani Physiotherapists
Manzoor1, Alam Zeb2, Arif Shah3, Ali Rahman4
1 Physical Therapist, Islamabad Club, Islamabad, Pakistan
2 PhD Scholar, University of Hasselt, Belgium
3 Physical Therapist, Paraplegic Centre, Peshawar, Pakistan
4 Assistant Professor, Khyber Medical University Islamabad Campus, Islamabad, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2025130410
ABSTRACT:
Background: Physiotherapists play an important role in the rehabilitation of post-operative Anterior Cruciate Ligament Reconstruction (ACLR). Return to Sport after ACLR is one of the primaries aims of the patients.
Objective: This survey aimed to define the present clinical treatment approach of Pakistani physiotherapists for treating ACLR patients and find out the standards used for return to sports after ACLR.
Methodology: An online questionnaire consisting of four separate sections, demographic data, and medical practice about ACLR post-operative therapy comprising the parameters for return to sports was used to survey Pakistani physiotherapists. Descriptive analysis was performed for demographic and professional characteristics of the physiotherapists.
Results: Out of 1375, 710 physiotherapists responded to the questionnaire. The response rate was 51.6%. Two-hundred and eighteen (40.4%) physical therapists showed that post-ACLR rehabilitation should be started lower than one-week post-surgery, 48.1% recommended that therapy be initiated between one and two weeks and 11.5% said beginning it later three or more weeks. The standards used for return to sports allowance standards were associated to physical aspects such as quadriceps strength (76.5%), hamstring strength (69.1), hip muscle strength (66.3%), and knee ROM (65.1%). A few therapists used functional (17%) and psychological (18.1%) characteristics of their clients to support return to sports choice.
Conclusion: The study showed that the majority of the physiotherapists focused on the parameters related to physical factors for return to sports and a small number worked on the self-reported functional scale and psychological parameters.
Keywords: Anterior Cruciate Ligament, Physiotherapists, return to sports
Introduction:
Anterior Cruciate Ligament (ACL) ruptures/injuries are the most common, especially during return to sports involving landing and pivoting movements. The annual incidence of ACL ruptures is 68.6 per 100,000 people every year.1 The standard clinical treatment for ACL rupture is surgical ACL reconstruction (ACLR).2 The main aims of ACLR is to maximize knee functional capacity and stability, whilst allowing a safe return to sport (RETURN TO SPORTS).3 The primary outcome after ACLR is return to sports. So, physiotherapists must practice authenticated methods and parameters to decide the patient capacity for return to sports.4-6
The standard for return to sports allowance commonly used by physiotherapist engaged in the recovery of patient’s post -ACLR is the quantity of time after operation, as it replicates curing and graft development.7-10 Further standards for return to sports are required to confirm that the patient undergoing ACLR is capable of enduring the physical loads usually enforced during return to sports activities.5, 11-13 According to a study, 13% of the literature took objective parameters for return to sports, 32% used a time centered, and 40% didn’t suggest any standards.8, 14 While parameters and standards used to decide return to sports post ACLR have been broadly examined in recent years, there is a substantial deviation in the available recommendations.11, 15-18 Some literature only assessed functional and physical factors, snubbing potential psychological features involved in return to sports.16, 17 A few literature focus on the parameters of knee joint slackness for assessment making about return to sports.15, 18
Though there is no agreement, the most commonly suggested standards to evaluate the preparedness for return to sports post-ACLR are based on: quads and hamstring power, enactment during functional examinations , client described functional result parameters , and psychological preparedness.14, 16, 18, 19 Thus, these procedures should be normally implemented during the post-ACLR rehab practice. The judgment about a person’s preparedness should be made by the professionals who are frequently involved in treating post-ACLR patients.12, 19 Recent data from Australians, Americans, and Brazilian physiotherapists specify significant dissimilarities in the parameters and objective standards used to explain preparedness for return to sports post-ACLR.20, 21 Currently, no data is available about the clinical experience and standards used by the physiotherapists to define preparedness for return to sports in Pakistan. Therefore, this survey aimed to define the present practice used by physiotherapists in the management of post-ACLR and find out the standards used for return to sports after ACLR.
Methodology
The survey was accepted by the ethical board of School of Health Sciences (Ref. No 462/2023/ADM/SHS). The total numbers of registered physiotherapist with the Pakistan Physical Therapy Association (PPTA) are 1375 according to the World Physiotherapy. We included all of them in our survey. An online questionnaire consisting of four separate sections was used to review Pakistani therapists. The questionnaire was adopted Brazilian study.22 Section 1 contained information regarding purpose and procedures; section 2 informed consent forms; section 3 demographic and professional data; and section 4 was related to clinical practice regarding ACLR post-operative treatment containing the parameters /standards used to define return to sports. Physiotherapists working in Pakistan for at least one year in private and government tertiary care hospitals were included in our study. Those physiotherapists who were working on an academic side and had not treated ACLR patients were excluded from this study. The questionnaire was distributed for completion through E-mails, WhatsApp, and Facebook groups between April 1, 2023, and September 1, 2023. The estimated time for questionnaire completion was about 10-15 minutes.
After survey closure, the responses were saved to an Excel sheet from Google Forms and then exported to SPSS 22 for investigation. Descriptive statistics was performed for the demographic and qualified characteristics of the physiotherapists. The answers about experimental experience post-ACLR along with the return to sports standards were investigated by means of frequency and percentage parameters.
Results
Out of 1375, 710 physiotherapists responded to the questionnaire. The response rate was 51.6%. Of 710 physiotherapists only 540 fulfilled our inclusion standards. Tables 1 and 2 showed data on demographics and medical training of the physiotherapists, respectively. There were nearly equivalent numbers of males 276(51.1%) and females 264 (49.9%) and the bulk of the physiotherapists (84.07%) were below the age of forty (mean age = 34.8 ±7.9 years). Most of the physiotherapists (30.2%) lived in Punjab followed by Sindh (29.6%), Khyber Pakhtunkhwa (21.3%), and Baluchistan (18.9%). One-hundred seventy-three (32.03%) physical therapists had experience between 5-8 years in treating post-ACLR rehabilitation, and practiced individual sessions (61.8%) for recreational athletes (50%) or amateur athletes (40%). The majority of the physical therapists (79.2%) did not have a domain in return to sports Physical Therapy.
Two-hundred and eighteen (40.4%) physical therapists reported that post-ACLR rehabilitation should be started less than 1-week post-discharge, 48.1% recommended that rehab be initiated amid 1-2 weeks after discharge while 11.5% said starting it after three or more weeks. Regarding return to sports clearance, 63.7% of physical therapists showed that the decision was to be made by a multidisciplinary team, 25.1% reported the decision should be made by the physical therapists and 11.2% responded the decision was to be made by the orthopedic surgeon.
The maximum time duration recommended by the physical therapists for off return to sports were 1-3 period of months (10.3%), 4-5 period of months (19.8%), 6-7 period of months (42.5%), 8-9 months (21.6%), and 10-12 months (5.5%).
Only 5.9% of the physical therapists did not mention any precise standards for return to sports approval. Maximum of the return to sports consent standards/parameters were related to physical aspects and the bulk of the physiotherapists stated numerous uses of quadriceps strength (76.5%), hamstring strength (69.1), hip muscle strength (66.3%), and knee ROM (65.1%) (Figure 1).
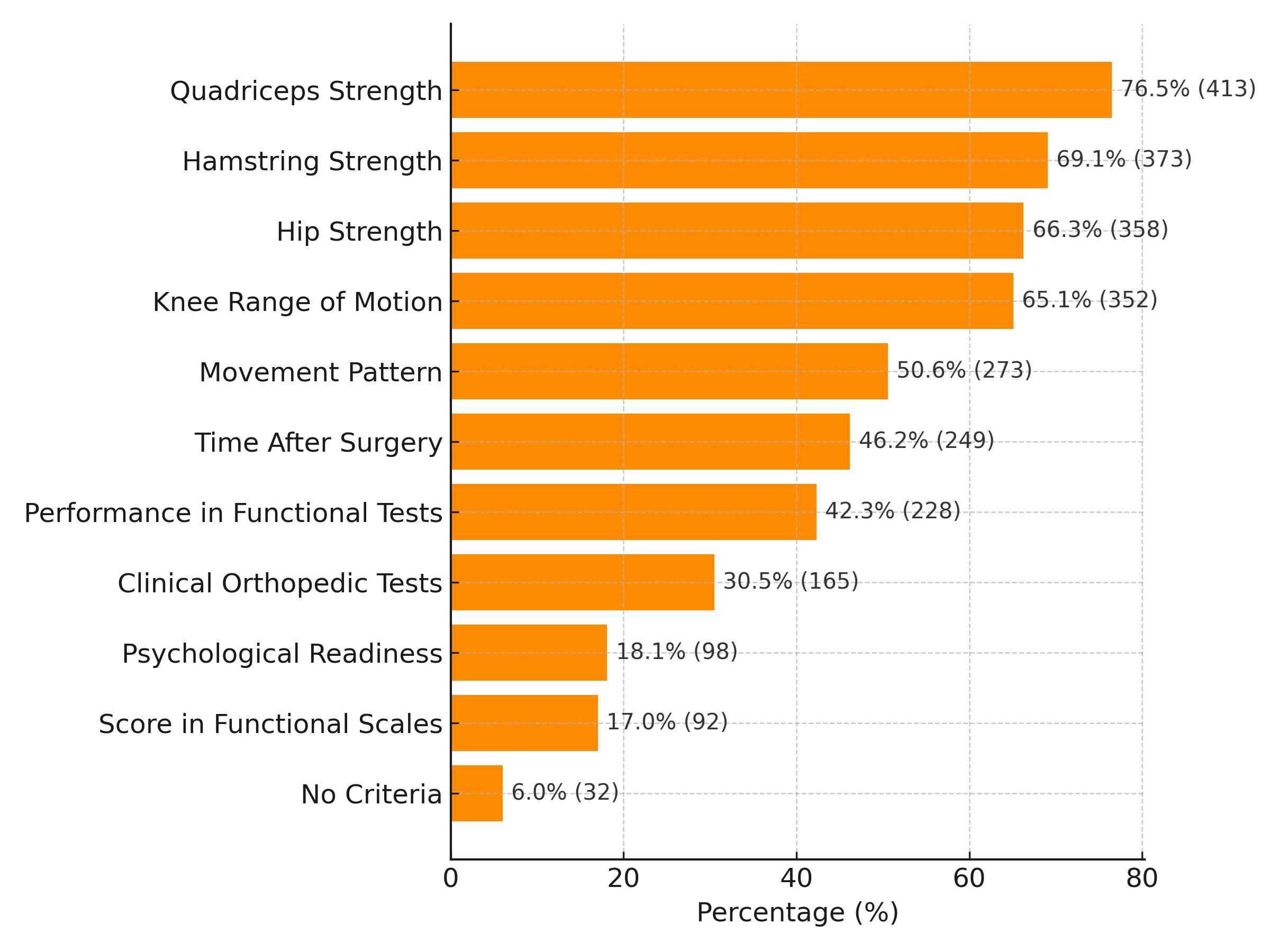
Figure 1: Standards used by Pakistani Physiotherapists to decide preparedness for return to sports
| Table 1 Demographic profile of Physiotherapists | |
| Variable | Frequency N (%) |
| Gender | |
| Male | 276 (51.1%) |
| Female | 264 (49.9%) |
| Age | |
| 21-30 years | 184 (34.1%) |
| 31-40 years | 270 (50%) |
| 41-50 years | 65 (12.1%) |
| 51-60 years | 21 (3.1%) |
| Above 60 years | 0 (0%) |
| Mean ± standard deviation | 34.8 ± 7.9 years |
| Province | |
| Khyber Pakhtunkhwa | 115 (21.3%) |
| Punjab | 163 (30.2%) |
| Sindh | 160 (29.6%) |
| Baluchistan | 102 (18.9%) |
| Education | |
| DPT | 291 (54.1%) |
| Master | 248 (45.9%) |
| PhD | 1 (0.1%) |
| Table 2: Professional characteristics of the Physical Therapists | |
| Variables | Frequency N (%) |
| Amount of experience with ACLR rehabilitation | |
| 1-4 Years | 158 (29.2%) |
| 5-8 Years | 173 (32.1%) |
| 9-12 Years | 98 (18.2%) |
| Above 12 Years | 111 (20.5%) |
| Mean ± standard deviation | 8.6 ± 6.4 years |
| Job settings | |
| Tertiary Care Hospital | 276 (51.1%) |
| (Both Private and Public sectors) | |
| District Headquarter Hospital | 264 (49.9%) |
| Patient’s activity level | |
| Sedentary patients | 39 (7.3%) |
| Recreational Athlete | 243 (50%) |
| Amateur Athlete | 217 (40%) |
| Professional Athlete | 41 (7.6%) |
| Treatment types Post-operative ACLR | |
| Individual | 28 (5.3%) |
| Collective | 334 (61.8%) |
| Collective and Individual | 178 (32.9%) |
| Time to start ACLR post-operative rehabilitation | |
| Less than 1 week | 218 (40.4%) |
| 1-2 weeks | 260 (48.1%) |
| 3 or more weeks | 62 (11.5%) |
| Responsible for defining return to sports clearance | |
| Physical Therapist | 136 (25.1%) |
| Orthopedic Surgeon | 60 (11.2%) |
| Multidisciplinary Team | 344 (63.7%) |
| Off sports/return to sports | |
| 1-3 Months | 56 (10.3%) |
| 4-5 Months | 107 (19.8%) |
| 6-7 Months | 230 (42.5%) |
| 8-9 Months | 117 (21.6%) |
| 10-12 Months | 30 (5.5%) |
| Certificate in sports Physiotherapy | |
| Yes | 428 (79.2%) |
| No | 112 (20.8%) |
Discussion
Clinical reviews and evidence-based guidelines on post-ACLR rehabilitation often stipulate a range of early actions that should be started in the first post-operative week, many of which are not delivered to patients proceeding hospital discharge. These exercises bond with the early post-operative objectives and, given the significance of early swelling control, patella mobility, quality quadriceps activation and near-normal ambulation, as well as returning good knee range of motion (flexion and extension).23, 24 In a study carried out in Australia on post-ACLR rehabilitation, the conclusions exposed that physical therapists have changing inclinations for the timing of their initial sessions with patients after hospital discharge. About 27.8% of physical therapists favor to see their patients within the first 1-4 days following surgery, while 25.6% opt for a consultation at the 7-day mark, and another 30.5% favor a consultation between 7-14 days after the surgical procedure. Additionally, 15.3% of therapists specified that they wish to see patients once they have received consent from the surgeon to start outpatient rehabilitation.25 In another study, it was found that 38.5% of physical therapists desire to begin post-ACLR rehabilitation within one week after hospital discharge, while 47.8% stated that they normally start rehabilitation between 1 and 2 weeks post-ACLR. Moreover, 13.7% of therapists directed that they endorse starting of rehabilitation after three weeks.22 This study showed that 40.4% of physical therapists wanted to start rehabilitation in less than one week, 48.1% stated to start within 1-2 weeks post-ACLR, and 11.5% opted to begin rehabilitation after three or more week.
Standards and parameters for preparedness for return to sports after ACLR would not be limited to physical examination. It must also include an assessment of the player’s psychological & functional status.6, 12 In the present study, 18% of the physical therapists focused on the evaluation of psychological preparedness and 17.1% on functional scores which showed similarity with a Brazilian study.22 In compare to the current study, a study established that nearly 90% of the Australian physiotherapists considered psychological preparedness as a measure of the standards to begin return to sports post-ACLR.25 The use of recommended parameters has not focused on the physical aspects only but also on psychological and functional status. Therefore, this study showed an extensive gap between the clinical experience of Pakistan therapists and the recommended literature standards.
The quantity of time post-ACL is measured an important criterion for return to sports. Traditionally, the recommended period for return to sports is 6 months.5 Though, a study disclosed that, after 6 months of post-ACLR, near 51% decrease occur in the new injuries of knee. As the risk of injuries reduces after 9 months of operation, this is the time-period suggested preceding for return to sports.16 The majority of the authors are contrary to an quick return to sports post-ACLR.16, 26, 27 A review on revisualization method in human ACLR showed that this organic process lasts for more than 6 months.10 But, this study showed that 27.1% of the physical therapists recommended a stay away from return to sports for eight or further months, presenting the lack of devotion of Pakistani therapists to the utmost current references.
The time required for return to sports post-ACLR would not be the single criteria accompanied to assess a patient’s preparedness. 6, 15, 18, 19 The coming back to unobstructed return to sports activities is an important part of rehabilitation.28 Therefore, physical therapists ought to perform an inclusive assessment.6, 15, 18, 19 The current survey presented that maximum physiotherapists gave importance to physical factors to find the patients preparedness for return to sports. Moreover, 30.2% of physiotherapists used special tests as a factor for return to sports which showed similarity with Aquino et al 31.8%.22 Though, special tests (i.e. anterior drawer & Lachman tests) provide information about strength of the knee joint, not giving evidence about patient physical and functional aspects.29, 30
A few authors suggest the annexation of a Landing Error Scoring System , that evaluate the movement design during jumping, as a criterion that might specify the preparedness for patient return post-ACLR.15, 18 Almost more than half (51.3%) of the therapists suggested movement designs as parameter for return to sports in the present study. However, there is still a lack of consensus on its inclusion in return to sports clearance standards. Performances in functional tests are often suggested as an approach to objective assessment of the functional result of ACLR and standards of return to sports.15, 18, 31, 32 The current study reported that 42.3% of the physical therapists used functional assessments for return to sports approval. The likely reasons for this might be a dearth of information about functional tests or the time necessary to execute these assessments.
Amongst the major standards commended in the research for return to sport, a small number of physiotherapists (17.1%) used self-report functional questionnaire score. But, tools, such as the Knee Outcome Survey Activities of Daily Living Scale (KOS-ADLS) and the International Knee Documentation Committee (IKDC) individual form, should be used to support in detailing functional position from the patient perception.14, 16, 33-35 An agreement of professionals specified the IKDC survey as a key portion of the self-reported knee task to explain achievement post-ACLR and ligament injury.19 Moreover, IKDC values greater than the 15th centile score of unharmed individuals were projected as a parameters for return to sports.15, 18, 33, 35 So, parameters linked to the patient functional status evaluation should involve an extra inclusive evaluation of the person’s preparedness for return to sports.
This was the first survey related to the clinical practice pattern of ACLR rehabilitation and standards for return to sports in Pakistani physical therapists. The above-mentioned results might help physical therapists to focus on the suggested standards for return to sports.
Conclusion
This study is the first to portray the practice patterns of the physiotherapists responsible for the management of patients’ post-ACLR rehabilitation and return to sports. Majority of the therapists focus on the parameters related to physical attributes (i.e. muscle strength & range of motion) for return to sports, and a small number of physiotherapists work on the self-reported functional scale and psychological parameters for return to sports.
References
- Sanders TL, Maradit Kremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. The American journal of sporeturn to sports medicine. 2016;44(6):1502-7.
- Shea KG, Carey JL, Richmond J, Sandmeier R, Pitts RT, Polousky JD, et al. The American Academy of Orthopaedic Surgeons evidence-based guideline on management of anterior cruciate ligament injuries. JBJS. 2015;97(8):672-4.
- Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British journal of sporeturn to sports medicine. 2011;45(7):596-606.
- Feucht MJ, Cotic M, Saier T, Minzlaff P, Plath JE, Imhoff AB, et al. Patient expectations of primary and revision anterior cruciate ligament reconstruction. Knee Surgery, Sporeturn to sports Traumatology, Arthroscopy. 2016; 24:201-7.
- Barber-Westin SD, Noyes FR. Objective standards for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: a systematic review. The Physician and sporeturn to sportsmedicine. 2011;39(3):100-10.
- Van Melick N, Van Cingel RE, Brooijmans F, Neeter C, van Tienen T, Hullegie W, et al. Evidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. British journal of sporeturn to sports medicine. 2016;50(24):1506-15.
- Barber-Westin SD, Noyes FR. Factors used to determine return to unrestricted sporeturn to sports activities after anterior cruciate ligament reconstruction. Arthroscopy: the journal of arthroscopic & related surgery. 2011;27(12):1697-705.
- Bauer M, Feeley BT, Wawrzyniak JR, Pinkowsky G, Gallo RA. Factors affecting return to play after anterior cruciate ligament reconstruction: a review of the current literature. The Physician and sporeturn to sportsmedicine. 2014;42(4):71-9.
- Joreitz R, Lynch A, Rabuck S, Lynch B, Davin S, Irrgang J. Patient-specific and surgery-specific factors that affect return to sport after ACL reconstruction. International journal of sporeturn to sports physical therapy. 2016;11(2):264.
- Claes S, Verdonk P, Forsyth R, Bellemans J. The “ligamentization” process in anterior cruciate ligament reconstruction: what happens to the human graft? A systematic review of the literature. The American journal of sporeturn to sports medicine. 2011;39(11):2476-83.
- Davies GJ, McCarty E, Provencher M, Manske RC. ACL return to sport guidelines and standards. Current reviews in musculoskeletal medicine. 2017; 10:307-14.
- Dingenen B, Gokeler A. Optimization of the return-to-sport paradigm after anterior cruciate ligament reconstruction: a critical step back to move forward. Sporeturn to sports medicine. 2017; 47:1487-500.
- Narducci E, Waltz A, Gorski K, Leppla L, Donaldson M. The clinical utility of functional performance tests within one-year post-acl reconstruction: a systematic review. International journal of sporeturn to sports physical therapy. 2011;6(4):333.
- van Meer BL, Meuffels DE, Vissers MM, Bierma-Zeinstra SM, Verhaar JA, Terwee CB, et al. Knee injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: which questionnaire is most useful to monitor patients with an anterior cruciate ligament rupture in the short term? Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2013;29(4):701-15.
- Gokeler A, Welling W, Zaffagnini S, Seil R, Padua D. Development of a test battery to enhance safe return to sporeturn to sports after anterior cruciate ligament reconstruction. Knee surgery, sporeturn to sports traumatology, arthroscopy. 2017; 25:192-9.
- Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. British journal of sporeturn to sports medicine. 2016;50(13):804-8.
- Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge standards before return to sport is associated with a four times greater risk of rupture. British journal of sporeturn to sports medicine. 2016;50(15):946-51.
- Welling W, Benjaminse A, Seil R, Lemmink K, Zaffagnini S, Gokeler A. Low rates of patients meeting return to sport standards 9 months after anterior cruciate ligament reconstruction: a prospective longitudinal study. Knee Surgery, Sporeturn to sports Traumatology, Arthroscopy. 2018; 26:3636-44.
- Lynch AD, Logerstedt DS, Grindem H, Eitzen I, Hicks GE, Axe MJ, et al. Consensus standards for defining ‘successful outcome’after ACL injury and reconstruction: a Delaware-Oslo ACL cohort investigation. British journal of sporeturn to sports medicine. 2015;49(5):335-42.
- Ebert JR, Edwards P, Yi L, Joss B, Ackland T, Carey-Smith R, et al. Strength and functional symmetry is associated with post-operative rehabilitation in patients following anterior cruciate ligament reconstruction. Knee Surgery, Sporeturn to sports Traumatology, Arthroscopy. 2018; 26:2353-61.
- Greenberg EM, Greenberg ET, Albaugh J, Storey E, Ganley TJ. Rehabilitation practice patterns following anterior cruciate ligament reconstruction: a survey of physical therapists. Journal of Orthopaedic & Sporeturn to sports Physical Therapy. 2018;48(10):801-11.
- Aquino CF, Ocarino JM, Cardoso VA, Resende RA, Souza TR, Rabelo LM, et al. Current clinical practice and return-to-sport standards after anterior cruciate ligament reconstruction: a survey of Brazilian physical therapists. Brazilian Journal of Physical Therapy. 2021;25(3):242-50.
- Wilk KE, Arrigo CA. Rehabilitation principles of the anterior cruciate ligament reconstructed knee: twelve steps for successful progression and return to play. Clinics in sporeturn to sports medicine. 2017;36(1):189-232.
- Adams D, Logerstedt D, Hunter-Giordano A, Axe MJ, Snyder-Mackler L. Current concepts for anterior cruciate ligament reconstruction: a criterion-based rehabilitation progression. journal of orthopaedic & sporeturn to sports physical therapy. 2012;42(7):601-14.
- Ebert JR, Webster KE, Edwards PK, Joss BK, D’Alessandro P, Janes G, et al. Current perspectives of Australian therapists on rehabilitation and return to sport after anterior cruciate ligament reconstruction: A survey. Physical Therapy in Sport. 2019; 35:139-45.
- Capin JJ, Khandha A, Zarzycki R, Manal K, Buchanan TS, Snyder‐Mackler L. Gait mechanics and second ACL rupture: implications for delaying return‐to‐sport. Journal of Orthopaedic Research. 2017;35(9):1894-901.
- Nagelli CV, Hewett TE. Should return to sport be delayed until 2 years after anterior cruciate ligament reconstruction? Biological and functional considerations. Sporeturn to sports medicine. 2017;47(2):221-32.
- Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR. Recent advances in the rehabilitation of anterior cruciate ligament injuries. journal of orthopaedic & sporeturn to sports physical therapy. 2012;42(3):153-71.
- Tagesson S, Öberg B, Kvist J. Static and dynamic tibial translation before, 5 weeks after, and 5 years after anterior cruciate ligament reconstruction. Knee Surgery, Sporeturn to sports Traumatology, Arthroscopy. 2015; 23:3691-7.
- Ardern CL, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, et al. 2016 Consensus statement on return to sport from the First World Congress in Sporeturn to sports Physical Therapy, Bern. British journal of sporeturn to sports medicine. 2016;50(14):853-64.
- Reid A, Birmingham TB, Stratford PW, Alcock GK, Giffin JR. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Physical therapy. 2007;87(3):337-49.
- Engelen-van Melick N, van Cingel RE, Tijssen MP, Nijhuis-van der Sanden MW. Assessment of functional performance after anterior cruciate ligament reconstruction: a systematic review of measurement procedures. Knee Surgery, Sporeturn to sports Traumatology, Arthroscopy. 2013; 21:869-79.
- Logerstedt D, Di Stasi S, Grindem H, Lynch A, Eitzen I, Engebretsen L, et al. Self-reported knee function can identify athletes who fail return-to-activity standards up to 1 year after anterior cruciate ligament reconstruction: a delaware-oslo ACL cohort study. Journal of Orthopaedic & Sporeturn to sports Physical Therapy. 2014;44(12):914-23.
- Logerstedt D, Grindem H, Lynch A, Eitzen I, Engebretsen L, Risberg MA, et al. Single-legged hop tests as predictors of self-reported knee function after anterior cruciate ligament reconstruction: the Delaware-Oslo ACL cohort study. The American journal of sporeturn to sports medicine. 2012;40(10):2348-56.
- Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ, Committee IKD. The International Knee Documentation Committee subjective knee evaluation form: normative data. The American journal of sporeturn to sports medicine. 2006;34(1):128-35.
| Copyright Policy
All Articles are made available under a Creative Commons “Attribution-NonCommercial 4.0 International” license. (https://creativecommons.org/licenses/by-nc/4.0/). Copyrights on any open access article published by Journal Riphah college of Rehabilitation Science (JRCRS) are retained by the author(s). Authors retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means; provided the article is correctly cited. JRCRS does not allow commercial use of the articles published. All articles published represent the view of the authors and do not reflect the official policy of JRCRS. |