
Original Article: JRCRS. 2025; 13(4):210-214
4- Comparison of Passive Translatoric Intervertebral Glides and Manual Segmental Traction in patients with Mechanical Low Back pain: A Randomized Controlled Trial
Mahnoor Zia1, Zainab Noor Qazi2, Sana Javaid3, Huma Mehrin Khan4, Shakeel Ahmad5
1 Physiotherapist, Aziz Bhatti Hospital, Gujrat, Pakistan
2 Lecturer, Margalla Institute of Health Sciences, Islamabad, Pakistan
3 Consultant physical therapist, Healing Hands Mega Medical Complex Rawalpindi, Pakistan
4 Physiotherapist, Behavior and Special Education Services (BASES), Rawalpindi, Pakistan
5 Lecturer, Department of Physical Therapy and Health Rehabilitation, Al Jouf University, Sakkaka, Saudi Arabia.
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2025130404
ABSTRACT:
Background: Low back pain is a global health issue and leading cause of disability. It is frequently treated by using manual treatments in physiotherapy clinics including mobilizations and spinal traction.
Objective: To determine and compare the effects of joint mobilizations and manual spinal traction on pain, disablity and joint range of motion in mechanical low back pain
Methodology: In the Physiotherapy Department of Aziz Bhatti Hospital, Gujrat, 34 participants with the complaint of diagnosed and confirmed cases of mechanical low back pain, aged 25 to 65 years were split into two equal groups for a randomized clinical trial. Group A received Passive Translatoric Intervertebral Glides while Group B received Manual Lumbar Traction (MLT) and both received conventional core stability exercises. Data was gathered using Numeric Pain Rating Scale (NPRS), Modified Oswestry Diability Index (MODI), and a universal goniometer at baseline, 2nd week and 4th week using Non-probability convenient sampling technique. SPSS version 22 was used for data analysis. (Clinical Trial Registry Number: NCT05522543)
Results: A significant improvement in pain, disability and range of motion was seen in both groups at the 4th week of intervention (p<0.001). However, Group B (MLT) showed more improvement in NPRS compared with Group A (PTIG). Both the treatment groups including PTIG (p<0.001) and MLT (p=0.000) showed significant reduction in disability scores however no statistically significant difference was found in inter-group analysis for disability score (p=0.274), Flexion(p=0.610) or Extension (p=0.170).
Conclusion: The study concluded that both treatments are effective in lowering the pain, disability and improving lumbar range of motion. However, significant improvement was found in group B in reducing pain, while overall no significant group differences were observed.
Keywords: Joint range of motion, Mechanical low back pain, Mobilizations, Traction
Introduction:
Mechanical low back pain refers to the pain that arises from the spine, intervertebral structures like disc, nervous and soft tissues that include muscles and ligaments surrounding the area.1 The prevalence of low back pain is measured as 60%-84%.2 Mechanical low back pain is quite prevalent in all age groups from children to adults as well.3
The mechanism, by which low back pain develops, is stimulation of joint structure and surrounding soft tissues by a noxious stimulus which creates a nerve impulse that travels to the dorsal horn of the spinal cord via afferent pain fibers. The pain signals are processed there and travel up to the brain and thalamus via efferent fibers where these signals are translated and pain is perceived locally in that specific region. This whole process is mediated by A delta and C pain fibers. These pain pathways are reversible with the removal of noxious stimuli.4
Management includes pharmacologic or non-invasive conservative treatment options and others include invasive procedures or surgery. Non-invasive treatment includes physical therapy techniques like spinal manipulation, massage or superficial heating with pharmacologic treatment support like non- steroidal anti-inflammatory drugs or muscle relaxants.5 Mobilization techniques are one of the most important manual therapy techniques that are used as a whole in any physiotherapy treatment.6 Spinal Traction is also commonly used for low back pain management. It removes the pressure from the spinal structures and provides neurophysiological effects such as pain modulation of nociceptive input.7 Spinal traction has three mechanical benefits that are Distraction of intervertebral joints to reduce compressive forces, stretching of posterior longitudinal ligament that creates centripetal force at the back of the joint and it creates a suction force that draws the intervertebral disc back to its position.8
Restricted Joint mobility and pain can be effectively managed by using Intervertebral Translatoric glides and lumbar manual segmental traction, but currently there is weak evidence proving one technique more effective than the other. Therefore, the goal of this study is to evaluate the efficacy of both the treatments in pain, restricted range of motion and disability in mechanical low back pain patients.
Methodology
The single blind randomized controlled trial was conducted at Aziz Bhatti Shaheed Teaching Hospital (DHQ) Gujrat, for time duration of 3 months i.e. from April 2022 to June 2022. The study was initiated after the approval from the Institutional Review Board and Ethics Committee of RCR&AHS with (Ref Number: RCRS/REC/01049). The non-probability convenient sampling technique was applied. Open Epi software version 3 was used to calculate the sample size by using mean and SD of disability index as variable. A total of 34 sample size was allocated for participation. Participants randomized using sealed envelope method by using a computer generator method.
Patients aged 25 to 65 year (both men and women) fulfilling the inclusion criteria of mechanical low back pain, restricted lumbar movements lasting for more than 3 months with muscle weakness less than 4/5 during manual muscle testing and no neurological deficits were included in this study. Those with history of inflammatory musculoskeletal disorders like ankylosing spondylitis and rheumatoid arthritis, history of taking medications for cardiac failure, pregnancy, acute trauma, malignancy, class II BMI were excluded.
Intervention Protocol: Both group A and B received supervised treatment for 3 days per week for consecutive 4 weeks. Total 12 sessions were given to both treatment groups. Group A received passive translatoric intervertebral glides and Group B received manual lumbar traction. Outcome measures were taken at baseline (before treatment) at 2nd week of treatment and finally at the end of the sessions at 4th week. Both Groups A and B received core stabilization exercises and stretches that included prone press ups, knee to chest exercises, bridges and cat and camel stretches (1 set 10 reps).9
Group A patients were treated at the start of the session with heating pads at the area of pain for approximately 10 minutes before mobilization. Patient was properly educated about correct posture techniques related to ADLs, weight lifting, prolonged sitting and sleeping. Patient was properly positioned to prone for PA central glides with therapist’s ulnar side of the hand over the spinous process of the vertebra above the painful vertebra. Therapist used the body weight and applied Postero-anterior force on selected spinous process by leaning their body over the vertebra and performed oscillatory movements to the area for 10 seconds.10 Same glides were performed on the sides of vertebra and transverse processes for 10 seconds. Total 5 sets of both central and transverse PA glides were performed. The session was ended with light core stabilizing exercises that included lumbar flexion (Knee to chest), lumbar flexion and extension in quadruped position (cat and camel stretches), bridges and prone press-ups (1 set of 10 repetitions). Whole session lasted for 30 to 40 minutes. Home plan was given that included above mentioned core stabilizing exercises (2 sets with 10 reps)
Group B received Manual Lumbar traction for 3 days per week for a total duration of 4 weeks. Patient was educated about the posture correction and proper lifting techniques along with correct sitting and sleeping positions. Heating pad was used on painful region for 10 minutes. Manual segmental traction was applied on lumbar region with the Patient supine lying with hip and knee flexion with a thin foam cushion under the body to prevent slip. (For 15sec to 20 sec daily in 5 sets). Therapist exerted traction by leaning backwards against a belt placed around his/her back or hip that is attached below the patient’s knees. The direction of pull was adjusted according to the patient’s comfort. Lumbar facet gapping (LFG) in side lying was applied with wedge under the painful segment. Lumbar rotational facet gapping (LRFG) with the patient in side lying with knees fully flexed. A wedge or towel roll was used under the target vertebrae. Then patient is asked to rotate the upper body in contralateral direction.7 At the end of the session light core stabilizing exercises were performed that included lumbar flexion (Knee to chest), lumbar flexion and extension in quadruped position (cat and camel stretches), bridges and prone press-ups (1 set of 10 repetitions). Home plan was given to repeat the same exercises (2 sets with 10 reps). Whole session lasted for 30 to 40 minutes 3x a week.
Numeric Pain Rating Scale (NPRS) was used to assess the back pain intensity.11 Modified Oswestry Disability Index (MODI) was used to assess disability in patients with low back pain.13 Range of motion (ROM) was measured by using goniometer.12
Data was analyzed using SPSS version 22. Data was presented using the Consolidated Standards of Reporting Trials (CONSORT) checklist (Figure 1). Analytical analysis was based on normality testing for variables by Shapiro–Wilk test. The data was non-normally distributed (p>0.05) for pain, disability and ROMs so the non-parametric tests were used. For between group analysis, Mann Whitney U test was used and for within group analysis, Friedman Test was used. Threshold of the statistically significant difference was p value < 0.05 at confidence interval (CI) of 95%.
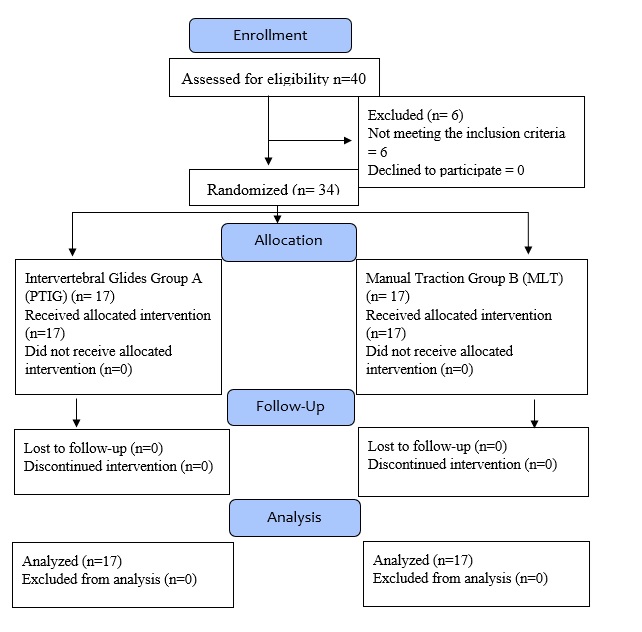
Figure 1: CONSORT Diagram showing Methodology
Results
34 patients with mechanical low back pain participated in this study of which 17 (50%) were in each of the two groups. There were 12(70.6%) females and 5(29.4%) males in Group A and 13(76.5%) females and 9(23.5%) males in group B. The mean age of the participants was 37.91±8.67 years.
A significant improvement in pain, disability and range of motion was seen in both groups at the 4th week of intervention (p<0.001). However, Group B (MLT) showed more improvement in NPRS compared with Group A (PTIG). Both the treatment groups including PTIG (p<0.001) and MLT (p<0.001) showed significant reduction in disability scores however no statistically significant difference was found in inter-group analysis for disability score (p=0.274), Flexion(p=0.610) or Extension (p=0.170).
| Table 1: Within Group Analysis (Friedman Test) | ||||
| Variables | Group A Median (IQ) |
p-value | Group B Median (IQ) |
p-value |
| Baseline NPRS | 8 (2) | <0.001 | 7 (2) | <0.001 |
| 2nd Week NPRS | 6 (2) | 5 (2.5) | ||
| 4th Week NPRS | 5(1.5) | 2 (2) | ||
| Baseline MODI | 34 (10) | <0.001 | 34 (12) | <0.001 |
| 2nd week MODI | 30 (14) | 28 (14) | ||
| 4th week MODI | 24 (14) | 20 (16) | ||
| Baseline Flexion | 51 (13.5) | <0.001 | 52 (11) | <0.001 |
| 2ndweek Flexion | 55 (8.5) | 55 (6) | ||
| 4th week Flexion | 60 (4) | 60 (5) | ||
| Baseline Extension | 20 (7.5) | <0.001 | 20 (7.5) | <0.001 |
| 2ndweek Extension | 22 (6) | 25 (5.5) | ||
| 4th week Extension | 25 (4) | 28 (5) | ||
| Table 2: Between Group Analysis (Mann Whitney U Test) | |||
| Variables | Group A
Median (IQ) |
Group B
Median (IQ) |
P-Value |
| Baseline NPRS | 8 (2) | 7 (2) | 0.339 |
| 2nd week NPRS | 6 (2) | 5 (2.5) | 0.193 |
| 4th week NPRS | 5 (1.5) | 2 (2) | 0.045 |
| Baseline MODI | 34 (10) | 34 (12) | 0.245 |
| 2nd week MODI | 30 (14) | 28 (14) | 0.205 |
| 4th week MODI | 24 (14) | 20 (16) | 0.274 |
| Baseline Flexion | 51 (13.5) | 52 (11) | 0.760 |
| 2nd week Flexion | 55 (8.5) | 55 (6) | 0.892 |
| 4th week Flexion | 60 (4) | 60 (5) | 0.610 |
| Baseline Extension | 20 (7.5) | 20 (7.5) | 0.245 |
| 2nd week Extension | 22 (6) | 25 (5.5) | 0.259 |
| 4th week Extension | 25 (4) | 28 (5) | 0.170 |
Discussion
This study compared the effects of two manual therapy techniques including passive translatoric intervertebral glides and manual segmental traction in mechanical low back pain population. The outcomes of the study included were pain intensity measured by NPRS, level of disability measured by MODI scale and range of motion including lumbar flexion and lumbar extension. To current literature, search the study is first to compare the effects of these two interventions in mechanical low back in terms of above-mentioned study outcome tools.
Regarding the first outcome of the study the pain intensity; between group comparison showed significant difference (p=0.045) between the group on 4th of intervention with more reduction of pain in Group B (manual segmental traction). However, when groups compared at pre-post analysis both groups revealed significant reduction in pain intensity from baseline to 4th week of intervention (P< 0.001). The study finding regarding the effect of pain intensity could be compared with previous literature such as a randomized control trial study conducted by Karimi et al (2017) on low back pain population reported that application of manual segmental traction on lumbar is significantly effective in reducing the pain (P<0.05) with larger treatment effect.14 Similarly, another study conducted by Diab AA et al (2012) reported that in chronic mechanical low back application of manual traction focusing on segmental aspect reduces the pain effectively (P<0.05).15
In the study the treatment effect of PA glide and manual traction was determined on disability level on MODI scale. Both the treatment groups including passive translatory intervertebral glides (p<0.001) and manual segmental traction (p<0.001) showed significant reduction in disability scores. However, no statistical difference was found in between group analysis to show any superior improvement in any of the group (p=0.274). This study finding is also explainable through findings of previous studies such as randomized control trial conducted by Hyunju Oh et al (2018) with objective to inspect the efficacy of manual segmental traction therapy on the pain intensity and modified Oswestry disability index of chronic back pain patients. The authors reported that significant reduction in both pain (P<0.05) and Oswestry disability index (P<0.05) was observed in experimental group with manual spinal traction.13 Likewise related to posterior anterior glide effectiveness Ikram et al (2018) declared that application of posterior anterior glide in no specific low back is effective to reduce the disability level (P<0.05).16
The next outcome of the study was related to range of motions at lumbar spine including lumbar flexion and extension. The within group analysis revealed that both the treatment groups including passive translatoric intervertebral glides (p<0.001) and manual segmental traction (p<0.001) showed significant improvement in lumbar flexion. However, no statistical difference was found in between group analysis to show any superior improvement in any of the group to improve the lumbar flexion (p=0.610).
While related to lumbar extension the results were similar as lumbar flexion that both the intervention groups were found significantly effective in improving the lumbar extension s compared to bassline and 2nd week of intervention at the end of 4th of intervention (P<0.001). As previously no statistical difference was found in between group analysis to show any superior improvement in any of the group to improve the lumbar extension (p=0.170). Previously various studies has reported the similar findings related to both types of interventions such as study by Karimi et al (2017) reported that lumbar flexion range of motion significant improvement (P<0.05) in back pain population.14 Moreover, Aliaa Diab et al (2012) has also concluded the similar findings after the intervention of lumbar segmental motion traction in chronic mechanical low back pain population that this intervention effectively improves the lumbar flexion.15 Furthermore, study conducted by Ali MN et al (2019) reported the efficacy of PA glide in low back population that PA glide is effective to improve lumbar flexion (P<0.01) and lumbar extension (P<0.01).17
A limitation of this research is that it was single centered study. The study was only single blinded randomized control trial with a small sample size of 34. Future research ought to consider studies with advanced outcome tools such as radiographically outcome tools. Beside mechanical low back pain, these techniques must be evaluated on other patient population such as lower cross syndrome and disc bulge patients. The conventional treatment might have affected the results of both treatments. Both the treatments should be evaluated individually without any conventional treatment involved.
Conclusion
The study found that both passive translatoric (PA) glides and manual lumbar traction were significantly effective in lowering the pain intensity, lowering the lumbar disability, improving lumbar flexion range of motion, and improving lumbar range of extension. Superior significant improvement was found in posterior anterior glide in aspect of reducing pain intensity, while overall no significant group differences were observed.
References
- Will JS, Bury DC, Miller JA. Mechanical low back pain. American family physician. 2018;98(7):421-8.
- Edwards J, Hayden J, Asbridge M, Magee K. The prevalence of low back pain in the emergency department: a descriptive study set in the Charles V. Keating Emergency and Trauma Centre, Halifax, Nova Scotia, Canada. BMC musculoskeletal disorders. 2018; 19:1-10.
- Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain. 2016;157(1):55-64.
- Oostinga D, Steverink JG, van Wijck AJ, Verlaan J-J. An understanding of bone pain: A narrative review. Bone. 2020; 134:115272.
- Qaseem A, Wilt TJ, McLean RM, Forciea MA, Physicians* CGCotACo. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Annals of internal medicine. 2017;166(7):514-30.
- Seo U-H, Kim J-H, Lee B-H, editors. Effects of Mulligan mobilization and low-level laser therapy on physical disability, pain, and range of motion in patients with chronic low back pain: a pilot randomized controlled trial. Healthcare; 2020: MDPI.
- Asiri F, Tedla J, Alshahrani M, Ahmed I, Reddy R, Gular K. Effects of patient-specific three-dimensional lumbar traction on pain and functional disability in patients with lumbar intervertebral disc prolapse. Nigerian journal of clinical practice. 2020;23(4):498-502.
- Outeda LR, Cousiño LAJ, Carrera IdC, Caeiro EML. Effect of the maitland concept techniques on low back pain: a systematic review. Coluna/Columna. 2022;21(2): e258429.
- Cairns MC, Foster NE, Wright C. Randomized controlled trial of specific spinal stabilization exercises and conventional physiotherapy for recurrent low back pain. LWW; 2006.
- Ali MN, Sethi K, Noohu MM. Comparison of two mobilization techniques in management of chronic non-specific low back pain. Journal of bodywork and movement therapies. 2019;23(4):918-23.
- Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. Journal of pain research. 2018:851-6.
- Ganzalez GZ, Costa LdCM, Garcia AN, Shiwa SR, Amorim CF, Costa LOP. Reproducibility and construct validity of three non-invasive instruments for assessing the trunk range of motion in patients with low back pain. Fisioterapia e Pesquisa. 2014;21(4):365-71.
- Grönblad M, Hupli M, Wennerstrand P, Järvinen E, Lukinmaa A, Kouri J-P, et al. Intercorrelation and test-retest reliability of the Pain Disability Index (PDI) and the Oswestry Disability Questionnaire (ODQ) and their correlation with pain intensity in low back pain patients. The Clinical journal of pain. 1993;9(3):189-95.
- Karimi N, Akbarov P, Rahnama L. Effects of segmental traction therapy on lumbar disc herniation in patients with acute low back pain measured by magnetic resonance imaging: a single arm clinical trial. Journal of back and musculoskeletal rehabilitation. 2017;30(2):247-53.
- Diab AA, Moustafa IM. Lumbar lordosis rehabilitation for pain and lumbar segmental motion in chronic mechanical low back pain: a randomized trial. Journal of manipulative and physiological therapeutics. 2012;35(4):246-53.
- Ikram A, Farooq N, Khan U, Muhammad A, Niaz M,Mehmood A. Effect of Postero-Anterior LumberSpine Mobilization versus McKenzie Press-Ups in Non-Specific Low Back Pain. Pakistan Journal ofMedical Health Sciences. 2021 Sep; 15(9): 1-3
- Ali MN, Sethi K, Noohu MM. Comparison of two mobilization techniques in management of chronic non-specific low back pain. Journal of bodywork and movement therapies. 2019;23(4):918-23
| Copyright Policy
All Articles are made available under a Creative Commons “Attribution-NonCommercial 4.0 International” license. (https://creativecommons.org/licenses/by-nc/4.0/). Copyrights on any open access article published by Journal Riphah college of Rehabilitation Science (JRCRS) are retained by the author(s). Authors retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means; provided the article is correctly cited. JRCRS does not allow commercial use of the articles published. All articles published represent the view of the authors and do not reflect the official policy of JRCRS. |