
Original Article: JRCRS. 2026:14(1):11-16
3-Effectiveness of McKenzie Neck Exercise Combined with Conventional Physical Therapy versus Conventional Physical Therapy Alone in Patients with Chronic Nonspecific Neck Pain: A Randomized Controlled Trial
Salman Khan1, Naeem Ullah2, Tahir Hafeez3, Ayesha Siddiqa Ali4, Asad Ullah Khan5, Mariyam Kifayat6
1 Physiotherapist, Peshawar Institute of Cardiology, Peshawar, Pakistan
2 Lecturer, Ahmad Medical Institute, Peshawar, Pakistan / Clinical physiotherapist, My Health Wellness Centre, Peshawar, Pakistan
3 Consultant physiotherapist, Center of Physiotherapy, City Hospital, Bahawalpur, Pakistan
4 Teaching Assistant, Rehman Medical Institute, Peshawar, Pakistan
5,6 Demonstrator, Institute of Health Sciences, Khyber Medical University, D.I. Khan, Pakistan
Full-Text PDF DOI: https://dx.doi.org/10.53389/JRCRS.2026140103
ABSTRACT:
Background: Neck pain is a common problem, commonly associated with poor posture, mechanical stress or trauma. It is often nonspecific, i.e. no underlying disease is detected. Neck pain may interfere with the normal life and result in a chronic ache. The goal of the effective treatments, the physical therapy and exercises, including McKenzie technique, is to relieve pain and restore mobility.
Objective: To identify the superior outcome between McKenzie exercises versus conventional physiotherapy versus conventional physical therapy on its own in reducing pain and enhancing functionality and cervical range of motion in patients with persistent nonspecific neck pain.
Methodology: The present study was designed as a randomized controlled trial (RCT) conducted in the Hayatabad Medical Complex, Peshawar. A total of 26 participants were included, with sample size calculated using G*Power software (effect size = 1.0, power = 80%, α = 0.05). Participants were randomly allocated into control and experimental groups using a lottery. The Control group participants were given conventional physiotherapy only, whereas the experimental group received conventional physiotherapy with the addition of the McKenzie exercise. The numerical pain rating scale was used for pain. The Neck Functional Disability Scale was used for functional disability, and cervical ranges were measured through a goniometer
Results: The mean age of the participants was 43.35 ± 10.19 years. Male participants were 16 (61.5 %) and female participants were 10 (38.5 %). There were statistically significant differences in the NPRS score (p = 0.047), CNFDS score (p = 0.042), cervical flexion range (p = 0.046), cervical extension range (p = 0.035), cervical left rotation range (p = 0.025), cervical right rotation range (p = 0.051), cervical left lateral flexion range (p = 0.040) and cervical right lateral flexion range (p = 0.031) between control and experimental groups.
Conclusion: This study revealed that McKenzie exercises, along with conventional physiotherapy, are more effective at decreasing neck pain, and improving functionality, and cervical ROM than conventional physiotherapy alone in the context of chronic nonspecific neck pain. This advantage can be explained by the fact that the McKenzie method focuses on recurrent end-range movements and postural correction that assist in decreasing mechanical stress, centralizing pain, and increasing spinal mobility via active patient interaction.
Keywords: Chronic Non-specific neck pain, Copenhagen neck functional disability scale, McKenzie Exercise, NPRS.
Introduction:
Nonspecific neck pain is defined as neck pain for which no specific illness has been identified as the underlying cause of the complaint. In any location between the occiput and upper thoracic spine, it is characterized as a mechanical pain that affects muscles without a known reason. Muscles, joints, ligaments, intervertebral plates, and neural systems can cause nonspecific neck pain.1 Neck pain is common, with a projected lifetime prevalence of 67% among individuals aged 20 to 69 years.2 It is frequently caused by movements of the neck or prolonged neck postures, and it is often accompanied by a decreased range of motion (ROM) and a feeling of stiffness.4 In the working population, neck pain appears to be fairly persistent and recurrent; one year later, sixty percent to eighty percent of workers who experience neck pain still report having it.4 Six to twelve months after an accident, approximately half of those who have neck pain still have some level of neck pain.5 This stresses the persistent and repetitive character of nonspecific neck pain that is a major socioeconomic, as well as a functional, burden to people and health care systems in the world. Prognosis is important in making clinical decisions. A well-prognosing patient may simply need education and counselling on the contrary, a poorly-prognosing patient may need a comprehensive evaluation and specific treatment or intervention.6
The present management Physical therapy is thought to be the foundation of the management of chronic nonspecific neck pain. Rehabilitation is evidence-based and widely supported by exercise to manage chronic neck pain It involves manual therapy, stretching, strengthening, postural therapy, and education to re-establish health and minimize the intensity of pain. It is essential to use the evidence-based intervention strategy that can maximize patient outcomes and minimize the recurrence.7, 8, 9
Despite many studies that support the application of a therapeutic exercise in chronic neck pains, the best mode of exercise is still not clear.8 The McKenzie Method is a directional preference-based, mechanical diagnosis and therapy (MDT) technique that consists of directional preference exercises designed to facilitation self-treatment and postural correction designed by Robin McKenzie in the 1980s. It has been demonstrated to reduce pain and increase the range of motion of the spinal cord of patients with mechanical spinal disorders.8, 9 Nevertheless, there is a lack of studies comparing McKenzie exercises to traditional physiotherapy of chronic nonspecific neck pain. The majority of studies have either compared general exercise or electrotherapy modalities without combining the two concepts to achieve the best results. Thus, McKenzie exercise in combination with conventional therapy could also be better in pain relief, functional disability, and cervical mobility than conventional therapy itself.9 Thus, there are few data on its added value in patients with chronic nonspecific neck pain when it is used in conjunction with traditional physiotherapy. Consequently, the question that needs to be studied is whether this combination produces better results than traditional therapy or not.10
The research purpose of the present study was to compare the effect of McKenzie exercises along with conventional physiotherapy to conventional physiotherapy on the effect on pain, functional disability, and cervical range of motion in patients with chronic nonspecific neck pain. The combined treatment was theorized to yield more positive effects with respect to pain reduction and functional improvement and cervical mobility improvements in comparison to traditional physiotherapy only.
Methodology:
This randomized controlled trial (RCT) was conducted in accordance with the CONSORT 2010 guidelines over a period of six months, from April to October 2024, at the Hayatabad Medical Complex (HMC-MTI), Peshawar. Ethical approval was obtained from the Graduate Committee (GC) of the Institute of Physical Medicine and Rehabilitation (IPM&R), Khyber Medical University (KMU), with Ethical Approval No. KMU(IPM&R)/MSPT/2024/80, followed by final approval from the Advanced Studies and Research Board (ASRB). Written informed consent was obtained from all participants before enrollment. The trial was prospectively registered with the Iranian Registry of Clinical Trials (IRCT) under registration number IRCT20230907059376N5.
The study included male and female patients aged 18 to 65 years, who were diagnosed with chronic nonspecific neck pain (duration ≥ 3 months) and a pain score ≥ 3 on the Numeric Pain Rating Scale (NPRS). Individuals with radiating pain, recent neck surgery, spinal cord lesions, serious pathologies (infection, inflammation, and malignancy), psychological disorders, those on neck pain medications, or those who received treatment in the past three months were excluded. A sample size of 26 participants (13 per group) was determined via G*Power software, with a calculated effect size of 1.0, power of 80%, and α = 0.05, on the basis of post-intervention NPRS scores from a previous study.11
The Participants were recruited via a consecutive sampling technique and randomly allocated into two groups (A and B) via the lottery method. Group A (control) was treated with conventional physiotherapy, which included hot packs (10 minutes), transcutaneous electrical nerve stimulation (TENS, 10 minutes), soft tissue release (5 minutes), and isometric neck exercises in 10 repetitions sets. Group B (experimental), was given the same conventional therapy and the McKenzie neck exercise protocol, but was intended to be given in gradual progressions during four weeks’ time, each week using particular techniques and frequencies.2,12 The sessions of the treatment model took around 40-45 minutes and were administered five days a week, in four weeks consecutively. The McKenzie exercise regime involved supine and sitting retraction exercises, overpressure extension exercises, and a combination of lateral flexion and rotation exercises with overpressure under the therapist assistance.13 The treatments were performed by licensed physiotherapists who had at least five years of clinical experience in musculoskeletal rehabilitation and McKenzie method certification.
The Outcome measures were NPRS for pin, Copenhagen Neck Functional Disability Scale (CNFDS) for functional disability, and a goniometer to measure cervical range of motion (ROM) during flexion, extension, lateral flexion, and rotation.14 15 All measurements were taken before and after intervention by a blinded assessor to ensure unbiased evaluation.16
The Data were analyzed via IBM SPSS version 26. Descriptive statistics were used to present demographic characteristics. The Shapiro-Wilk test was used to assess normality. Continuous data are expressed as means and standard deviations, while categorical data are presented as frequencies and percentages. Depending on normality, between-group comparisons were made using the Independent Sample T-test or the Mann-Whitney U test. A p-value ≤ 0.05 was considered statistically significant.
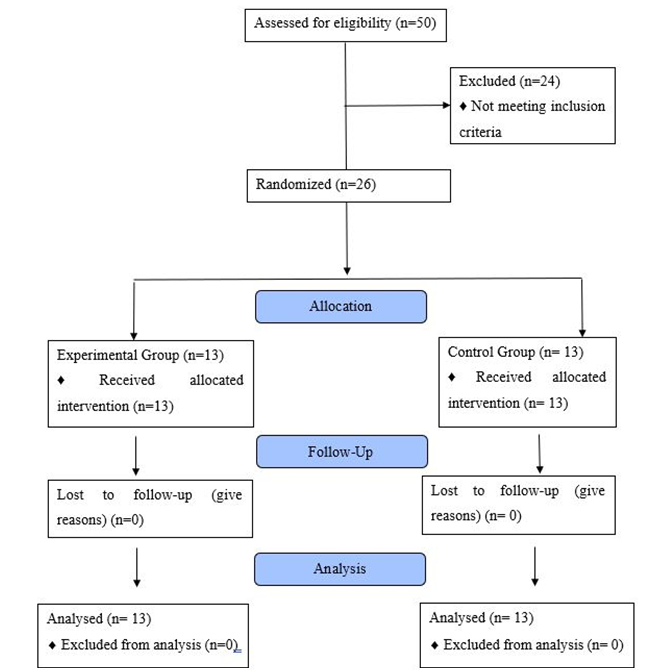
Figure 1: CONSORT Flow Diagram
Results:
In this study, sums of 26 participants were included. The mean age calculated was 43.35 ± 10.19 years. From these 26 patients, 16 (61.5%) were male, while the remaining 10 (38.5%) participants were female. On the basis of work status, mostly were working n = 20 (76.5%), followed by not working n = 5 (19.2%), and the remaining 1 (3.8%) participant was a student. Based on duration of pain, 13 (50%) had pain for 3 to 6 months, 7 (26.9%) had pain for 6 to 12 months, 4 (15.4%) had pain for 1 to 2 years, and 2 (7.7%) had neck pain for greater than 2 years.
Post – Intervention Scores NPRS, CNFDS and Range of Motion: Post-intervention assessment showed that in the control group, the mean NPRS score was 3.76 ± 0.83, with most participants (26.9%) reporting a pain level of 4/10. The mean CNFDS score was 16.07 ± 3.70. Cervical range of motion (ROM) measured via goniometer revealed mean values of 33.95 ± 1.83° for flexion, 35.61 ± 0.78° for extension, 36.10 ± 0.96° for left rotation, 37.16 ± 1.18° for right rotation, 35.86 ± 0.98° for left lateral flexion, and 35.97 ± 1.20° for right lateral flexion. In the experimental group, the mean NPRS score was also 3.76 ± 0.83, with the highest proportion (38.5%) reporting a pain score of 2/10, followed by 30.8% each for 3/10 and 4/10. The mean CNFDS score in this group was 14.69 ± 3.17. Post-intervention cervical ROM in the experimental group showed greater improvements, with mean values of 38.16 ± 0.74° for flexion, 40.01 ± 0.71° for extension, 42.11 ± 1.52° for left rotation, 41.75 ± 1.18° for right rotation, 38.02 ± 0.76° for left lateral flexion, and 40.53 ± 0.74° for right lateral flexion.
| Table 1: Demographic Data Inter-Group Comparison | |||||||
| Variables | Control group
(% / M ± S.D) |
Experimental group
(% / M ± S.D) |
Total | ||||
| Age (in years) | 43.69 ± 10.66 | 43 ± 10.09 | 43.35 ±10.19 | ||||
| Gender | Male | 8 | (30.8%) | 8 | (30.8%) | 16 | (61.5%) |
| Female | 5 | (19.2%) | 5 | (19.2%) | 10 | (38.5%) | |
| Duration of Pain | Pain for 3-6 months | 6 | (23.1%) | 7 | (53.8%) | 13 | (50.0%) |
| Pain for 6-12 months | 4 | (15.4%) | 3 | (23.1%) | 7 | (26.9%) | |
| Pain for 1-2 years | 2 | (7.7%) | 2 | (15.4%) | 4 | (15.4%) | |
| Pain since > 2 years | 1 | (3.8%) | 1 | (7.7%) | 2 | (7.7%) | |
| Table 2 Baseline Data Inter – Group Comparison Pain and ROMs | |||
| Variable | CG (M ± S.D) | EG (M ± S.D) | P value |
| Baseline NPRS Score | 5.85 ± 1.14 | 6.38 ± 1.39 | 0.649 |
| Baseline CNFDS Score | 20.15 ± 5.16 | 22.08 ± 4.09 | 0.416 |
| Baseline Cervical Flexion | 33.03 ± 1.94 | 33.95 ± 1.93 | 0.258 |
| Baseline Cervical Extension | 35.02 ± 1.44 | 34.56 ± 1.41 | 0.355 |
| Baseline Cervical Left Rotation | 36.48 ± 1.55 | 36.47 ± 1.55 | 0.865 |
| Baseline Cervical Right Rotation | 35.98 ± 1.79 | 35.03 ± 1.91 | 0.814 |
| Baseline Cervical Left Lateral Flexion | 35.95 ± 1.58 | 34.84 ± 1.66 | 0.903 |
| Baseline Cervical Right Lateral Flexion | 34.84 ± 0.79 | 34.97 ± 1.24 | 0.212 |
| Table 3: Post – Intervention Control and Experimental Groups NPRS, CNFDS and Cervical ROMs Data Demographics | |||||
| Variables | Control Group | Experimental Group | |||
| N | Mean ± S.D / % | N | Mean ± S.D / % | ||
| NPRS Score | 13 | 3.76 ± 0.83 | 13 | 2.92 ± 0.86 | |
| 2 / 10 | 1 | 3.8% | 5 | 38.5% | |
| 3 / 10 | 3 | 11.5% | 4 | 30.8% | |
| 4 / 10 | 7 | 26.9% | 4 | 30.8% | |
| 5 / 10 | 2 | 7.7% | 0 | 0 % | |
| CNFDS Score | 13 | 16.07 ± 3.70 | 13 | 14.69 ± 3.17 | |
| Cervical ROM | Neck Flexion | 13 | 33.95 ± 1.83 | 13 | 38.16 ± 0.74 |
| Neck Extension | 13 | 35.61 ± 0.78 | 13 | 40.01 ± 0.71 | |
| Neck Left Rotation | 13 | 36.10 ± 0.96 | 13 | 42.11 ± 1.52 | |
| Neck Right Rotation | 13 | 37.16 ± 1.18 | 13 | 41.75 ± 1.18 | |
| Neck Left Lateral Flexion | 13 | 35.86 ± 0.98 | 13 | 38.02 ± 0.76 | |
| Neck Right Lateral Flexion | 13 | 35.97 ± 1.20 | 13 | 40.53 ± 0.74 | |
| Table 4: Post – Intervention Pain and Neck ROMs Inter – Group Comparison | |||
| Variable | CG (M ± S.D) | EG (M ± S.D) | P-value |
| Post – Intervention NPRS score | 3.76 ± 0.83 | 2.92 ± 0.86 | 0.047 |
| Post – intervention CNFDS score | 16.07 ± 3.70 | 14.69 ± 3.17 | 0.042 |
| Post – Intervention Neck Flexion | 33.95 ± 1.83 | 38.16 ± 0.74 | 0.046 |
| Post – Intervention Neck Extension | 35.61 ± 0.78 | 40.01 ± 0.71 | 0.035 |
| Post – Intervention Neck Left Rotation | 36.10 ± 0.96 | 42.11 ± 1.52 | 0.025 |
| Post – Intervention Neck Right Rotation | 37.16 ± 1.18 | 41.75 ± 1.18 | 0.051 |
| Post – Intervention Left Lateral Flexion | 35.86 ± 0.98 | 38.02 ± 0.76 | 0.040 |
| Post – Intervention Right Lateral Flexion | 35.97 ± 1.20 | 40.53 ± 0.74 | 0.031 |
Discussion:
The main aim of this RCT was to assess the effectiveness of McKenzie exercises in the non-specific neck pain (NP) in relation to conventional physical therapy. The intervention group showed statistically significant pain reduction and cervical range of motion (ROM) and functionality improvement when compared with the control group, which serves as a clinical benefit of the use of McKenzie exercises as a component of regular physiotherapy. The findings of the current research are similar to other researches which have examined the benefits of McKenzie exercises on non-specific neck pain. Kjellman et al.17 and Abbass et al.18 also found that McKenzie therapy had significant pain reliever and cervical ROM in patients who have undergone McKenzie therapy indicating the effect of this therapy on neuromuscular control and functional recovery in patients with cervical correction and re-education of cervical stabilizers.17 Our combined method had better outcomes than that of McKenzie and therapeutic exercises used in the study by Lytras et al. (2017), who also discovered both as effective in treating chronic neck pain. This suggests that the multimodal method can apply the centralization effect and mechanical loading concept of McKenzie method, which contributes to restoring the intervertebral disc, and the peripheral nociceptive input, thereby providing better functional results.19
When compared to the study of Arshad et al., which compared the McKenzie extension exercises with the neck isometric exercises in non-specific neck pain, our findings again reinforce the idea that using McKenzie principles as a part of conventional therapy may enhance the deep cervical flexor, increase segmental stability and hasten the pain centralization. Although Arshad et al. demonstrated positive changes in pain and cervical range of movement (ROM), in our Group B the mean changes in NPRS scores and CNFDS scores were higher, which supports the physiological usefulness of combined intervention strategies.
As a major factor of reducing pain, Kim et al. highlighted posture correction. In line with this, our findings indicate that McKenzie based movements enhance spinal extension and neutral position, which reduces the strain of the cervical muscle and promotes adaptive neuromuscular re-education.21
We find consistency with more recent meta-analyses by Kjellman et al. (17), and Kumar et al.22 which find that McKenzie therapy is significantly more effective than passive modalities in improving ROM as well as reducing the intensity of pain, in particular when the McKenzie therapy is applied in conjunction with active exercise programs. This enhances the body of evidence that supports the implementation of combined interventions in the treatment of chronic nonspecific neck pain treatment.23 These findings are supported by recent systematic reviews. In a 2022 meta-analysis, Al-Khayer et al. determined that McKenzie therapy is very effective at the reduction of pain and disability in chronic neck pain compared to conventional care. The other review Eom et al. (2023) completed claimed that McKenzie exercises are associated with improved cervical proprioception and postural orientation, which also supports our findings.
These results indicate that physiotherapists need to consider the combination of McKenzie exercises with traditional modalities in order to have a faster and more holistic recovery among patients with chronic nonspecific neck pain. This integrated strategy is cheap, easy, and applicable in both the clinical and domestic rehabilitation units. Although the current research offers important data on the efficiency of the McKenzie exercises in conjunction with traditional physical therapy, the limitations are to be mentioned. Long-term follow-up is also a limitation and future studies have to look at the maintenance of pain relief and motor control adaptation after the intervention. The improvements in pain, ROM and functionality should also be followed up to determine whether the research will be sustained in the future. Moreover, this research was dedicated to general non-specific neck pain, and it would be interesting to see what McKenzie exercises can do to particular subtypes of neck pain, i.e. postural or muscle strain.
Conclusion:
The results of this paper have shown that McKenzie exercises, when administered with the traditional physiotherapy, are better than traditional physiotherapy in reducing neck pain, functional ability and cervical range of motion. These findings offer good clinical support to the use of McKenzie exercises as part of the usual physiotherapy. The method does not only improve the pain relief and cervical mobility but also improves the postural correction and functional recovery in the long term. Consequently, McKenzie exercises as a non-invasive intervention to the standard treatment approach may represent a convenient and cost-efficient recommendation to physiotherapists in treating chronic, non-specific neck pain.
References:
- Bussieres AE, Stewart G, Al-Zoubi F, Decina P, Descarreaux M, Hayden J, et al. The treatment of neck pain–associated disorders and whiplash-associated disorders: a clinical practice guideline. 2016;39(8):523-64. e27.
- Neeraj K, Shiv VJBJMHR. To Compare the Effect of Strengthening Neck Exercise and Mckenzie Neck Exercise In Neck Pain Subject. 2016;3(10):69.
- Kumar S, Kumar N, PraveShen S, Kumar R, Sharma NJEJoM, Medicine C. Compare the effectiveness of McKenzie Techniques and Isometric Strengthening Exercise In Patients with Cervical Radiculopathy. 2021;7(11):4679-91.
- Tunwattanapong P, Kongkasuwan R, Kuptniratsaikul VJCr. The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: a randomized controlled trial. 2016;30(1):64-72.
- Verwoerd M, Wittink H, Maissan F, de Raaij E, Smeets RJJMS, Practice. Prognostic factors for persistent pain after a first episode of nonspecific idiopathic, non-traumatic neck pain: a systematic review. 2019;42:13-37.
- Blanpied PR, Gross AR, Elliott JM, Devaney LL, Clewley D, Walton DM, et al. Neck pain: revision 2017: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. 2017;47(7):A1-A83.
- Chen X, Coombes BK, Sjøgaard G, Jun D, O’Leary S, Johnston VJPt. Workplace-based interventions for neck pain in office workers: systematic review and meta-analysis. 2018;98(1):40-62.
- Arribas-Romano A, Fernández-Carnero J, González-Zamorano Y, Rodríguez-Lagos L, Alguacil-Diego IM, Molina-Álvarez M, et al. Manual Therapy Effects on Nonspecific Neck Pain Are Not Mediated by Mechanisms Related to Conditioned Pain Modulation: A Randomized Clinical Trial. 2023;12(12):3894.
- Rodríguez-Lagos L, Alguacil-Diego IM, Molina-Álvarez M, Tejera DM, Mercado-Romero F. Manual Therapy Effects on Nonspecific Neck Pain Are Not Mediated by Mechanisms Related to Conditioned Pain Modulation: A Randomized Clinical Trial. 2023.
- Naz S, Jamali N, Iftikhar A, Nawaz H, Iqbal T, Ghafoor. Compare the Effectiveness of Mulligan (Nags & Snags) and McKenzie (Self-Stretching) On Improving the Pain and Functional Ability in Patient with Chronic Neck Pain: Effectiveness of Mulligan and McKenzie in Patient with Chronic Neck Pain. 2023:47-52.
- Arshad N, Ahmad A, Ali B, Imran M, Hayat SJKMUJ. Comparison between McKenzie extension and neck isometric exercises in the management of nonspecific neck pain: a randomized controlled trial. 2020;12(1):6-9.
- Abdel-Aziem A, Mohamed R, Draz A, Azab A, Hegazy F, Diab RJERfM, et al. The effect of McKenzie protocol vs. deep neck flexor and scapulothoracic exercises in subjects with chronic neck pain–a randomized controlled study. 2022;26(9).
- Enwemeka CS, Bonet IM, Ingle JA, Prudhithumrong S, Ogbahon FE, Gbenedio NAJJoO, et al. Postural correction in persons with neck pain. II. Integrated electromyography of the upper trapezius in three simulated neck positions. 1986;8(5):240-2.
- Misterska E, Jankowski R, Glowacki MJBmd. Cross-cultural adaptation of the Neck Disability Index and Copenhagen Neck Functional Disability Scale for patients with neck pain due to degenerative and discopathic disorders. Psychometric properties of the Polish versions. 2011;12:1-8.
- Cleland JA, Childs JD, Whitman JMJAopm, rehabilitation. Psychometric properties of the Neck Disability Index and Numeric Pain Rating Scale in patients with mechanical neck pain. 2008;89(1):69-74.
- Jordan A, Manniche C, Mosdal C, Hindsberger C. The Copenhagen Neck Functional Disability Scale: a study of reliability and validity. J Manipulative Physiol Ther. 1998;21(8):520-7.
- Kjellman G, Oberg B. A randomized clinical trial comparing general exercise, McKenzie treatment and a control group in patients with neck pain. J Rehabil Med. 2002;34(4):183-90.
- Abbass M, ul Qamar S, Habib M, Hanif M, Masood S, Usman H. A Study to Compare the Effectiveness of McKenzie Neck Exercise and Contract Relax Stretching in Mechanical Neck Pain. Journal of Health and Rehabilitation Research. 2024;4(2):1629-33.
- Lytras D, Koulis N, Sykaras E. Comparison of two Exercise Programs in Patients with Chronic Neck Pain. 2017.
- Arshad N, Ahmad A, Ali B, Imran M, Hayat S. Comparison between McKenzie extension and neck isometric exercises in the management of nonspecific neck pain: a randomized controlled trial. Khyber Medical University Journal. 2020;12(1):6-9.
- Kim S, Jung J, Kim N. The effects of McKenzie exercise on forward head posture and respiratory function. The Journal of Korean Physical Therapy. 2019;31(6):351-7.
- Kumar S, Kumar N, PraveShen S, Kumar R, Sharma N. Compare the effectiveness of McKenzie Techniques and Isometric Strengthening Exercise In Patients with Cervical Radiculopathy. European Journal of Molecular & Clinical Medicine. 2021;7(11):4679-91.
- Enwemeka CS, Bonet IM, Ingle JA, Prudhithumrong S, Ogbahon FE, Gbenedio NA. Postural correction in persons with neck pain. II. Integrated electromyography of the upper trapezius in three simulated neck positions. Journal of Orthopaedic & Sports Physical Therapy. 1986;8(5):240-2.
Copyright Policy All Articles are made available under a Creative Commons “Attribution-NonCommercial 4.0 International” license. (https://creativecommons.org/licenses/by-nc/4.0/). Copyrights on any open access article published by Journal Riphah college of Rehabilitation Science (JRCRS) are retained by the author(s). Authors retain the rights of free downloading/unlimited e-print of full text and sharing/disseminating the article without any restriction, by any means; provided the article is correctly cited. JRCRS does not allow commercial use of the articles published. All articles published represent the view of the authors and do not reflect the official policy of JRCRS.